


Over the last 35 years the concept of trauma as a public health issue has evolved, from the development of the National Centre for Post-Traumatic Stress Disorder for war veterans in the United States in 1989, to initiating research between 1995 and 1997 on the adverse childhood experiences (ACEs) (Felliti et al, 1998), which extended this health issue into the civilian world of children, young people and families who have been exposed to traumatic experiences such as abuse and neglect. The plethora of evidence from this study (Fellliti et al, 1998) identified the ‘lifelong detrimental physical, emotional and mental health effects experienced by individuals with a history of trauma’ (Cannon et al, 2020: 1). This resulted in the development of a strengths-based approach known as trauma-informed care in 2005, which aims to promote a culture of safety, empowerment and healing (Tello, 2018).
A traumatic experience has been defined as: ‘an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life threatening’ (The Substance Abuse and Mental Health Services Administration [SAMHSA], 2014a: 7). Trauma is insidious and can occur as a result of many different experiences, which are often subdivided into two different types. Type one trauma refers to an individual experiencing a single incident such as an assault, rape or a serious accident. Type two trauma refers to persistent experiences such as child or domestic abuse, trafficking or the context of war (SAMHSA, 2014a). Some individuals may experience both types of trauma, this is otherwise known as compound or complex trauma (Maguire et al, 2009); however, it is not the incidence or experience which determines the type of trauma, it is the symptoms which the individual is experiencing (Brewin et al, 2017).
Evidence suggests that children and young people who experience trauma and adversity at an early age, are more likely to experience poor mental and physical health, misuse substances (e.g. alcohol and drugs), be involved in the criminal justice system and experience early mortality (Ashton et al, 2016; Bellis et al, 2015). It is estimated that ‘a third of young people in the United Kingdom (UK) have experienced trauma during childhood and adolescence, which doubles their risk of experiencing a range of mental health conditions such as depression, conduct disorder, alcohol dependence, self-harm and suicide’ (Torjesen, 2019: 1854). Furthermore, there is already evidence that ‘50% of all lifelong mental health disorders develop in young people by the age of 14, and 75% begin by the age of 24 years' (Kessler et al, 2005: 593).
Trauma informed education
School nurses have a key public health role through the universal and targeted services they provide across education and health, providing a link between school, home and the community (Royal College of Nursing [RCN], 2020). Therefore, they have a fundamental role in working with children and young people who have experienced trauma, through their ability to develop positive and trusting therapeutic relationships (Feo et al, 2017). As they are always available to provide support, as well as being understanding, empathetic, genuine, non-judgemental and self-aware, while still maintaining clear professional boundaries and providing a quality service (Dziopa and Ahern, 2009). Hence, they are in a unique position to support and deliver the six key principles of a trauma-informed approach with children and young people, these being (SAMHSA, 2014:10):
- Safety
- Trustworthiness and transparency
- Peer support, collaboration and mutuality
- Empowerment/voice/choice
- Cultural/historical/gender issues.

However, due to the complexity of adverse childhood experiences and trauma, a coordinated response is needed with other services and agencies such as the criminal justice system, social care, education, and the police to provide a population health approach, as it does not just impact the individual, but also their relationships, community and wider society (Magruder et al, 2017). Therefore, we need to develop a trauma-informed workforce, which begins by integrating trauma informed education within all professional training programmes, as it is evident that it is still in its infancy within the field of nursing, in comparison to other professions such as psychiatry, social work and psychology (Li, 2019). This will ensure we keep pace with the continual change to health-care practice (Kermansaravi et al, 2015) and prepare both the present and future generations of practitioners with the right knowledge, skills and behaviours, to address this public health issue.
Recently Higher Education Institutions (HEIs) have received approval for the delivery of the master's level Specialist Community Public Health Nursing (SCPHN) apprenticeship programmes in the UK (Institute for Apprenticeships and Technical Education, 2020). Aligned to this, the Nursing and Midwifery Council (NMC, 2020) has also proposed the development of new SCPHN Standards of Proficiency, which provides an ideal opportunity for universities and educators to develop new and review existing curricula for future programmes.
So, the aim of this article is to consider integrating trauma informed education within SCPHN training programmes, utilising a life-course approach, by focusing on adolescence—which is a sensitive period of development, where the ‘leading causes of death in this age group relate to risk taking behaviours and trauma’ (Roberts et al, 2020: 25)—by utilising the four R's (key assumptions) of a trauma-informed approach as the key components of this education framework (SAMHSA, 2014: 9):
- Realise
- Recognise
- Respond
- Re-traumatisation.
Realise
The proposed curriculum would encompass a combination of theoretical frameworks, these being life-course epidemiology, psychosocial epidemiology and trauma-informed education. The initial stage of a trauma-informed approach ‘realise’ involves having an understanding of a young person's behaviour, experience and their coping strategies, therefore the foundations of this framework, will be centred on a life-course approach. The origins of life-course epidemiology overlap with psychosocial epidemiology as a result of medical and social research coming together to combine ‘biological programming, risk accumulation and health inequalities’ (Jacob et al, 2017: 5). Both theoretical frameworks will provide underpinning knowledge on the adolescent life course in which ‘neurobiology, psychological processes and social attachment interact’ (SAMHSA, 2014: 5).
The importance of adolescent health has become more widely recognised, as historically this has been a forgotten age group, despite the immense changes that occur in young people during this stage of their development (Kennedy, 2010). What is clear is that adolescents have distinct health and wellbeing needs in relation to that of younger children. As young people are vulnerable to a range of stressors, which have the potential to affect their biological, physical and emotional development. Similarly, this also applies to a range of social and environmental transitions such as relationships with peers, parents and carers and transitions within school, university/college, workplace.
Therefore, from a psychosocial perspective, the curriculum, will examine adolescent health behaviours, attachment, types of stress, a window of tolerance and risk and protective factors. This will be facilitated in conjunction with a life-course perspective, by reviewing the critical period model (Kuh et al, 2003), which considers the impact of exposure to risks having a lifelong effect on a young person's development. Other models such as accumulation of risk and chains of risk model (Kuh et al, 2003) provide an extension on the critical period model, by considering the multiple effects of exposure to risks (behavioural, environmental and socio-economic) as a result of trauma, which may result in one bad experience or risk leading onto another.
Recognise
The second stage of a trauma-informed approach is ‘recognise’, where the focus will shift to a combination of trauma-informed theory and life-course epidemiology in which a historical overview of trauma-informed care, adverse childhood experiences study (Felliti et al, 1998) and types and signs of trauma will be provided. Consequently, there will be more emphasis on the neurobiological effects of brain plasticity within adolescence, which also considers the different brain trajectories for both males and females and the impact of this, on behaviour and development (Kanwal et al, 2016). The impact of a traumatised brain can have immense effects, on an individual's day-to-day functioning, as an overactivated amygdala (responsible for emotions) within the brain, is the reason why the body is in constant state of high alert for danger (Christie, 2018). In other regions of the brain, the prefrontal cortex (thinking centre) is underactivated, hence why individuals may experience difficulty concentrating and learning and the anterior cingulate cortex (empathy, impulse control) is also underactivated, which means young people may have difficulty managing their emotions (Wave Trust, 2018).
Respond
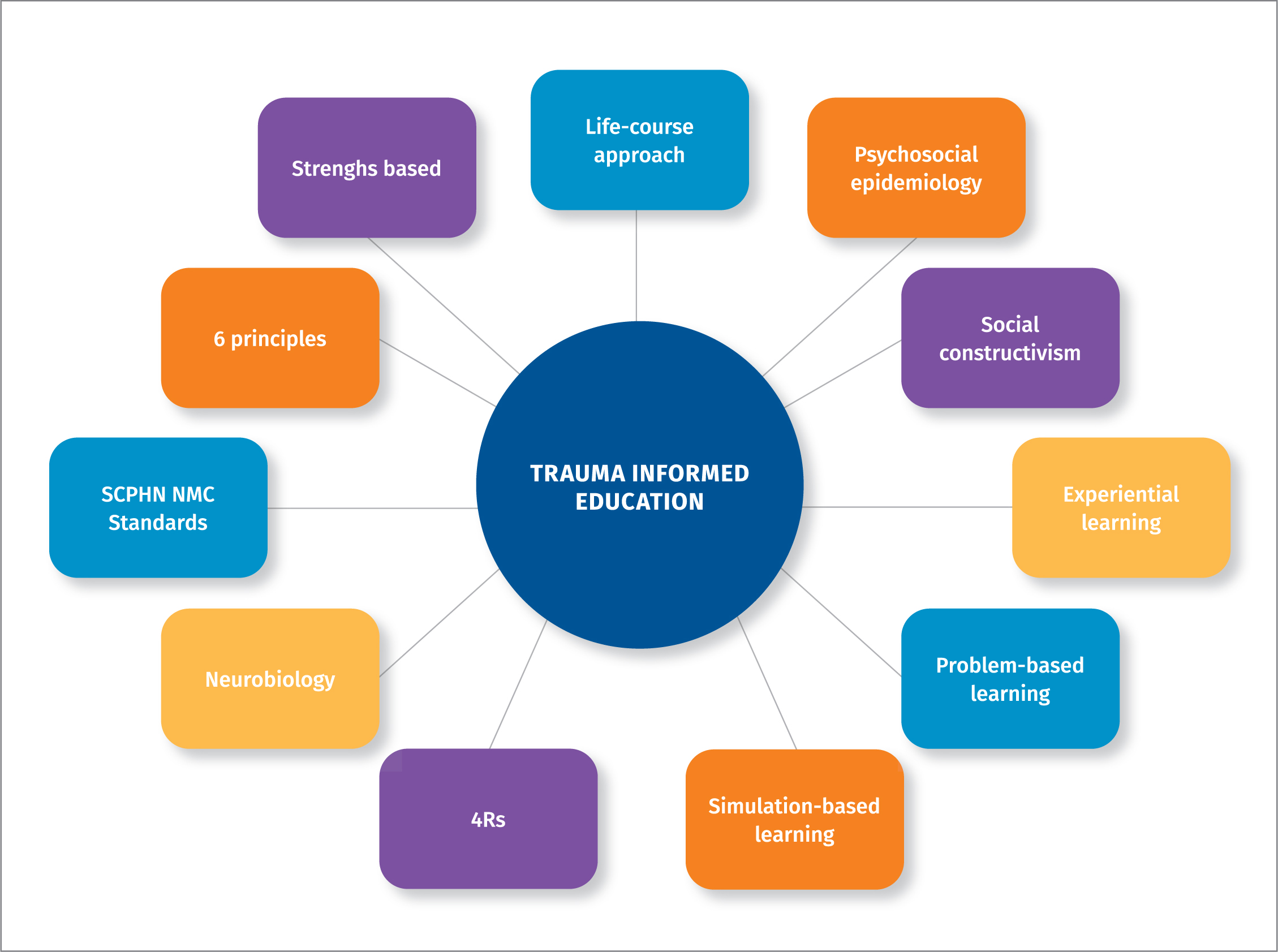
A strengths-based approach will be applied to the delivery of the curriculum, which changes the focus from ‘What is wrong with you’ to adopting a trauma lens by asking instead ‘what has happened to you’ (Sweeney et al, 2018:1). The purpose of this is to ensure that children and young people who have experienced trauma can feel safe and can gain trust, while also considering an asset-based focus, on identifying their own strengths as well as the support available around them to promote recovery. Aligned to this, social constructivism (Vygotsky, 1978) and experiential learning (Kolb, 1984) theories will provide the underpinning pedagogy, in order to integrate new knowledge on trauma into professionals existing knowledge and experience (Draper, 2013). Therefore, a range of teaching and learning strategies such as problem-based and simulation-based learning, reflection and action learning sets will be utilised (Figure 1). This will not only incorporate all learning styles (Honey and Mumford, 1982) but also encourage critical thinking, peer assessment, collaborative working and problem solving, all of which will be underpinned and supported by the SCPHN standards of proficiency (NMC, 2004).
Re-traumatisation
The focus of this stage is centred on integrating knowledge and skills of trauma-informed care into practice, from both a professional and organisation/service provider standpoint. This includes ensuring that school nurses have access to health and wellbeing support, should this be needed within both the university and practice setting. As exposure to people, places or situations may trigger a past trauma, which they have experienced in their own professional or personal life. This also reinforces the importance of clinical supervision and safeguarding supervision for school nurses in their role in practice, which not only provides ‘protected time to discuss the risks associated with their caseloads but is also an opportunity for them to address any anxieties or emotions’ they may have (Warren, 2018: 35). Furthermore, from an operational perspective, organisations should have a trauma-informed ethos within their policies and procedures, as well as ensuring trauma informed care pathways and ongoing training of all of their staff is fully in place.
Conclusions
Children and young people can experience trauma from an early age, the effects of this can have an impact on their development into adulthood and across the rest of their lifespan, if not addressed. School nurses have a central role in providing trauma informed care within their role in practice, as they are often a first port of contact for vulnerable children and young people who are distressed and in need of support. Therefore, it is essential that both current and future school nurses receive trauma-informed education, within their specialist practice training, to assist them in their key role in addressing this public health issue.