


Childhood immunisations protect infants, children and the wider community from infectious diseases that would otherwise be common in childhood (Parliamentary Office of Science and Technology, 2013). Every child in the UK is offered free immunisations as part of the National Immunisation Programme, which offers protection against 14 preventable and infectious diseases (Birmingham Community Healthcare, 2021). The Department of Health regularly amends the childhood immunisation schedule based on recommendations from The Joint Committee on Vaccination and Immunisation (JCVI), an independent scientific advisory body (Parliamentary Office of Science and Technology, 2013; UK Health Security Agency [UKSHA], 2020).
Sepsis is the leading cause of child morbidity and mortality, and immunisation remains the principal method of primary sepsis prevention (Plunkett and Tong, 2015). After immunisation, children are far less likely to contract the infection they have been vaccinated against and once enough people in the community are immunised, the infection can no longer spread so dies out (NHS England, 2018). Herd immunity occurs when a significant proportion of the population becomes immune (either through infection and recovery, or by vaccination) to a disease, making transmission from person-to-person unlikely and offering protection to the rest of the population. The proportion of a community which must be protected to achieve herd immunity differs between diseases, for example, measles ‘requires more than 95% of the population to be immune to stop sustained disease transmission and achieve herd immunity’ (Desai and Majumder:2113). Evidence has shown that some vaccinations, such as the Bacillus Calmette-Guérin (BCG) vaccine against tuberculosis (TB), can reduce (neonatal) mortality from infections other than TB ‘in a non-specific or pathogen agonistic manner’ (Aaby et al, 2011; Biering-Sørensen et al, 2017; Williamson et al, 2021:1887), providing additional benefits.
Parental consent is required for childhood immunisations in the UK, although the vaccination of children and young people against COVID-19 has raised wider questions about when adolescents can consent to vaccination. Parental consent can be overridden in some circumstances, which would usually require a ‘best interests’ decision by the courts. A child's immunisation is thus usually reliant on parental choice, yet some have argued that mandatory vaccination would be within the child's best interests (Wilkinson and McBride, 2021).
Parents with low confidence in childhood immunisations have reported a number of concerns around issues such as adverse effects (Stefanoff et al, 2010; Delkkosh et al, 2014), vaccination safety (Gust et al, 2005a; Gust et al, 2008; Stefanoff et al, 2010), vaccination-related pain (Delkosh et al 2014; Gust et al, 2005a; Gust et al, 2005b; Kennedy et al, 2011a) and persisting misperceptions regarding the immunisations, despite some parents adhering to the recommended immunisation schedules (Kennedy et al, 2011b). This in turn induces parental anxiety (Luthy et al, 2013) and is likely to increase the child's anxiety, potentially intensifying the pain experienced by children during the immunisation (Bearden et al, 2012). Studies have also revealed that a parent's personal experience of childhood immunisations had a greater influence on their choices than scientific evidence (Jones, 2012).
Vaccine hesitancy refers to a ‘delay in acceptance or refusal of vaccines, despite availability of vaccine services’ (MacDonald, 2015: 6163). Despite vaccines preventing 2–3 million deaths a year and being a cost-effective method of avoiding disease, in 2019 the World Health Organization (WHO) listed vaccine hesitancy as one of the top ten biggest threats to global health and predicted that a further 1.5 million deaths could be avoided if global coverage of vaccinations improved (WHO, 2019). In 2019, national coverage rates of childhood immunisations were falling and NHS Digital (2019) reported that 86.4% of 5-year-olds had completed their routine childhood immunisation schedule, and none of the routine immunisations met the 95% target adopted by the Department of Health and Social Care from the WHO.
The aim of this study is to undertake a systematic appraisal of evidence to explore how the uptake of childhood immunisations can be improved in England.
Rationale
The measles, mumps and rubella (MMR) vaccine was launched in the UK in 1988, when childhood immunisation uptake was at a 92% high (Raneri and Matusitz, 2014). Following the publication of a report by Wakefield et al (1998) which questioned the safety of the MMR vaccine and its potential links to autism, the rate of childhood immunisation dropped to 82% by 2003 and MMR outbreaks began to rise as a result of the allegation; the report was later retracted from The Lancet as it was considered fraudulent (Abhyankar et al, 2008). Coverage for the MMR vaccine then increased from 2007/08, peaking at 92.7% uptake for MMR vaccine by 24 months in 2013/14 (Ramsay, 2013). Yet, by 2018/19, coverage for all childhood immunisations for under-5s had declined and coverage for the MMR vaccine dose given at 1 year and 3 years 4 months (UKHSA, 2022) is currently at 85.5% (Rough, 2021). This figure is far lower than the 95% target recommended by the WHO to prevent a resurgence of measles and leaving the population at risk of contracting measles if they are exposed to the disease and not vaccinated against it.
Outbreaks of a disease can lead to a pandemic, which greatly increases morbidity and mortality within the geographical area, affirming the seriousness of mitigating against the risk of such outbreaks. Moreover, pandemics cause significant economic, social and political disruption, placing increased pressure on healthcare services, as well as periods of quarantine, infection fears, frustration, boredom, inadequate supplies, inadequate information and financial loss to individuals (Brooks et al, 2020). This, in turn, leads to higher rates of mental health problems among the population, which results in poorer health outcomes and increases the risk of premature mortality for those experiencing severe mental health disorders (WHO, 2015; Madhav et al, 2017; Zürcher et al, 2020).
The COVID-19 pandemic placed enormous stress on the NHS and despite the continued delivery of services to deliver childhood immunisations (in the earliest stages of the pandemic), vaccination rates across England reduced by between 19.8% and 25% in April 2019 and April 2020 (McDonald et al, 2020). As the COVID-19 pandemic continued and additional pressure was placed on primary care, there was an urgency to ensure that childhood immunisations remain a priority and children are up to date with their immunisations (Heffernan, 2020). The WHO (2020) recognises that strategies will require creativity and innovation but may in turn help to improve the overall quality of vaccination services. The Institute of Medicine (2004:4) defines health literacy as an individual's capacity to ‘obtain, process, and understand health information and services needed to make appropriate health decisions’ and older adults, adults of low educational attainment, racial and ethnic minorities, migrants and people with compromised health status are mostly likely to exhibit poor health literacy (Eichler et al, 2009). The COVID-19 vaccine is an essential means to establishing population immunity and reducing the spread of the coronavirus, though public hesitation around the vaccine has created major difficulties in relation to this and populations with a higher level of health literacy are less likely to exhibit vaccine hesitancy (Montagni et al, 2021; Biasio et al, 2021; Geana et al, 2021). Despite a lack of evidence, the recent decline in childhood immunisation uptake has been blamed on Covid vaccine fatigue among the public, as well as an increase in vaccine hesitancy as although COVID-19 vaccines have been found to be highly effective in preventing severe disease, they are less effective at preventing infection transmission and may have negatively effective parents' perceptions of the effectiveness of childhood immunisations (Bedford and Donovan, 2022).
The reasons for which people choose not to vaccinate are complex; however, a WHO advisory group identified them as being influenced by factors such as complacency, convenience and confidence (MacDonald, 2015). WHO (2019) categorises community health workers as the most trusted advisors and influencers on vaccination decisions and this review is thus likely to be of relevance and interest to community healthcare professionals working in England.
As a result of these findings, recommendations, and the current drop in childhood vaccination uptake, it was deemed relevant to pool a range of current evidence together and explore how childhood immunisation uptake can be improved in England.
Methods
Identifying the research question
The PICO tool was used to identify the research question and increase the reliability of the search (Table 1).
Table 1. PICO search terms
| Population | Childhood |
| Intervention | Immunisation, vaccination |
| Comparison | Increase |
| Outcome | Uptake, England |
Search strategy
A combination of three databases, CINAHL, Medline and Scopus, were electronically searched on the same date, 11th December 2021, using the following search terms “childhood” AND “immunisation” OR “vaccination” AND “increase” AND “uptake” AND “England” to reach maximum recall (Wright et al, 2015; Bramer et al, 2017).
Inclusion and exclusion criteria
Inclusion and exclusion criteria were applied to the papers yielded from the database search and grey literature obtained as part of this systematic review (Table 2).
Table 2. Inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
| Papers that discuss childhood immunisations | Papers that only discuss vaccinations in relation to adolescent or adult subjects |
| Papers published 2016–2021 | Papers published before 2016 |
| Studies conducted or papers published in England | International studies or those conducted in Wales, Northern Ireland or Scotland |
| Qualitative, quantitative and mixed methods research studies, secondary research | Narrative or descriptive papers |
| Papers that examine factors or discuss recommendations for how vaccine uptake can be improved | Papers that do not examine factors or discuss recommendations for how vaccine uptake can be improved |
| Peer-reviewed papers and studies | Non-peer-reviewed papers and studies |
| Papers/studies exploring routine childhood immunisations, offered to all | Papers/studies exploring vaccines offered only to specific patient groups, such as the BCG vaccine |
| Studies exploring general populations, such as studies completed within specific areas of the country. | Studies exploring specific patient groups, such as Gypsy, Roma and Traveller communities or children looked after. |
Literature sourced
This systematic review was undertaken in accordance with the criteria and principles adopted from Moher et al (2010) (see Figure 1). Each selected paper (see Table 3) was initially reviewed and summarised in an analytical matrix, which details each study's sample, design, strengths and limitations (see Appendices).
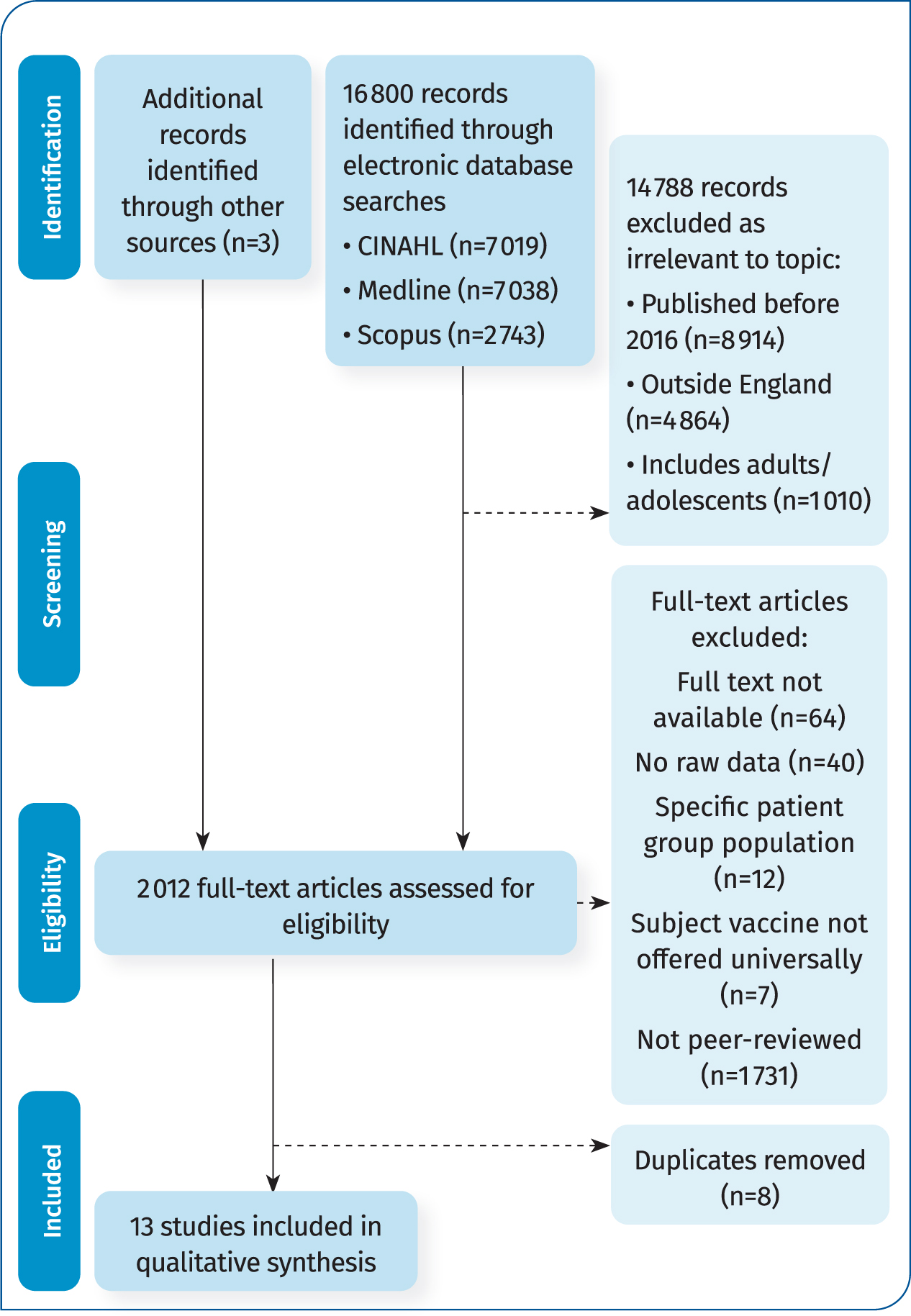
Table 3. An overview of the literature included
| Literature | Location, year and study design |
|---|---|
| Edelstein et al (2020) | England |
| 2012/13 and 2018/19 | |
| Mixed-methods study | |
| Crocker-Buque et al (2017) | England |
| May 2017 to February 2018 | |
| Mixed-methods study | |
| Christensen et al (2020) | South West England |
| September | |
| 2015–January 2016 | |
| Longitudinal study | |
| Quantitative | |
| Bell et al (2020) | England |
| Mixed-methods study | |
| April to May 2020 | |
| Paterson et al (2018) | Barnet, Bury, Leicestershire, and Surrey |
| March to June 2016 | |
| Cross-sectional qualitative study | |
| Lwembe et al (2016) | London |
| July 2012–February 2013 | |
| Qualitative evaluation study | |
| Smith et al (2017) | 2015-2016 Influenza Season |
| Cross-sectional online survey | |
| England | |
| Mixed-methods | |
| McGeown et al (2018) | London |
| February 2016 | |
| Qualitative study | |
| Santorelli et al (2020) | Bradford |
| March 2007–2014/15 | |
| Quantitative longitudinal study | |
| Sealey (2017) | Surrey |
| 2015/16–2016/17 | |
| Mixed-methods study | |
| National Institute for Health and Care Excellence (2017) | London |
| Public Health Guideline | |
| Rough (2021) | London |
| Research publication produced by UK Houses of Parliament Libraries to inform Members of the House of Commons and House of Lords | |
| NHS England and NHS Improvement (2019) | London |
| Findings from a review of immunisations and vaccinations |
Critique of the studies
Studies were assessed using widely-used appraisal tools, specifically developed to assess validity, relevance and applicability of published healthcare evidence (CASP, 2018; Hong et al, 2018) (see Appendices).
Discussion
The data identified was triangulated into five overarching themes:
- Forms of reminder and recall;
- Healthcare professionals and staff;
- Coordination
- Family-centred care
- Communication.
Forms of reminder and recall
Call and recall
Edelstein et al (2020) stated that forms of patient reminder and recall systems exist as one of the most effective interventions to improve vaccination uptake (Pereira et al, 2012; Harvey et al, 2015). Patient reminder and recall systems are a cost-effective method for families and children to be identified and notified that their immunisations are due or overdue and they can be delivered by various methods, such as via letter, telephone or text message (Jacobson, 2005; Williams et al, 2011; Centers for Disease Control and Prevention, 2016). Bell et al (2020) stated that such reminder and recall systems should be maintained, yet there is great variation between GP practices across the country in how reminder and recall systems are used (Crocker-Buque et al, 2017). Rough (2021) identified inconsistent reminder and recall as one of the key factors which negatively affects the uptake of childhood immunisations in England.
Reminder and recall systems are effective in combatting the common reasons for which immunisations are missed, such as parents and carers forgetting appointments or not being aware of the immunisation schedule, yet their success relies upon the accuracy of patient contact details, the completeness of vaccination and the viability of the contact method, in relation to the readability and comprehensibility of the message sent or given to each individual family, as well as the family's beliefs about vaccinations and their access to healthcare services (Pereira et al, 2012; Esposito et al, 2014). Children may miss vaccination for other reasons, such as illness, relocation (such as from a place where their health needs may have been neglected). The National Institute for Health and Care Excellence (NICE, 2009) and Kraszewski (2017) highlighted the importance of checking a child's vaccination status at every healthcare contact and providing the opportunity to generate a catch-up plan through an onward referral to an appropriate vaccination service or opportunistic vaccination before the family leave the premises. However, very limited evidence of opportunistic vaccination within the community exists, both within literature and anecdotally, despite these recommendations and the potential solutions to avoiding the barriers of children not being brought to planned appointments.
Escalating reminders
NHS England and NHS Improvement (2019) deem it more beneficial and proactive for general practices to utilise Reminder and Recall systems than opportunistic vaccination. Some practices have adopted a Reminder and Recall escalation process, in which patients will initially receive emails, texts or letters reminding them about vaccination and if they didn't respond, the system will escalate to administrative staff, then a nurse and finally a GP to phone a family to discuss and encourage them to book their child's vaccinations (McGeown et al, 2018). NICE (2009) that if a child does not attend, tailored reminder and recall invitations are sent and followed up by telephone or text message. NICE (2009) fail to specify what is meant by ‘tailored’ messages or invitations, though Kraszewski (2017) advises that consideration is given to a family's language and literacy levels, so on occasions, a telephone call may be more appropriate than a letter or text message reminder.
Text message reminders
During the 2019 general election campaign, the Conservative Party announced that it would introduce ‘a national vaccination reminder system to boost childhood vaccination rates’ so that ‘every family would receive a reminder from their GP practice that it is time for their child's next vaccinations’ (Rough, 2021:34). Bell et al (2020) found that parents are reportedly not receiving vaccination invites and reminders, which has worsened during and following the COVID-19 pandemic, when parents were unclear about whether vaccinations were still being offered, and the onus was on them to remember vaccinations were due and book their own appointment, exacerbated by the ‘stay home’ and ‘protect the NHS’ messages given by the government (Saxena, 2020). Particularly disproportionally affected by this (Public Health England [PHE], 2020) were Black and Asian Minority Ethnic (BAME) and low-income groups, placing them at risk of long-term health consequences as a result. Childhood immunisation uptake is generally lower among families of these groups (Forster et al, 2017) and additional targeted campaigns are needed (Bell et al, 2020) as they are often underrepresented in vaccination services, alongside those not registered with a GP.
Catch-up programmes
Catch-up programmes for MMR vaccines were urged by NHS England, following the UK's loss of its measles-free status in 2019 (Rough, 2021), and again in 2022 as MMR vaccination rates dropped to 85.5%, below the WHO's target of 95%. It remains unclear to what extent anti-vaccination sentiment around the COVID-19 vaccinations may have influenced this, though MMR vaccination rates are noted to be poorest in more deprived communities of the UK. Vaccine hesitancy is increasing in high income countries and practices often encounter patients who frequently do not attend appointments (vaccinations or otherwise) or respond to calls or letters. There is negligible evidence available on how to provide services and improve vaccine coverage for patients who frequently miss appointments or ‘are not brought’ and is identified as an opportunity for future research (Crocker-Buque et al, 2017).
Innovation
Alternative, simple, practice-based approaches can also be highly effective, such as birthday card reminders, verbal reminders during contacts, flagging children's electronic health records or checking siblings' vaccination status during GP visits (Kraszewski, 2017). Lwembe et al (2016) evaluated the use of a celebration card intervention to improve the uptake of childhood immunisations across nine boroughs of London. Healthcare professionals felt the initiative was positive and deliverable with current capacity and resource, though questions were raised about the sustainability of the programme, quantitative data collection and in relation to vaccine rejectors, on whom the scheme is unlikely to impact. The study concluded that the programme was valuable in its purpose as a form of reminder and recall, utilising theory and parental engagement to improve vaccination uptake, though further research is needed to quantitatively evaluate the effect of the programme on vaccination uptake, which will be challenging, given the number of other uncontrollable factors that influence uptake.
Healthcare professionals and staff
Staff roles
Delivering routine vaccinations results in an increased number of contacts for GP practices, alongside associated administrative tasks, reminder and recall activities and data input. This is combined with increased demand for GP services without increased funding or staffing (Baird et al, 2016), which presents a huge challenge. Nevertheless, healthcare professionals are highly trusted, and evidence strongly suggests that a vaccine recommendation or advice from a healthcare professional increases the likelihood of vaccination (Wiley et al, 2013). Health visitors, for example, are well placed to assess a family's vaccination status, proactively and positively promote immunisation and contribute to the delivery of a key public health intervention that prevents disease and prolongs life (Campbell et al, 2015). They have been singled out as the healthcare professionals with whom parents had the most positive experiences and had felt listened to (iHV, 2022), yet difficulties in accessing healthcare professionals in a timely manner has been identified as a factor which is negatively affecting the uptake of childhood immunisations (Rough, 2021). Furthermore, there remains a national shortage of around 5 000 health visitors (Day, 2022), reducing the capacity of a lot of health visiting services to complete this valuable work. Wilkinson (2022) also identifies the national shortage of health visitors as a factor which has influenced this figure, noting that vaccine uptake has in fact increased in Scotland, where a programme of 11 standard home visits is offered to families. This service offer provides an opportunity for public health discussion, a rapport to be built with families in order to gain trust. In comparison health visiting services in England currently only offer five mandated contacts, some of which may have been paused due to capacity issues and others may remain virtual (iHV, 2021). This can also significantly hinder a practitioner's ability to safeguard a vulnerable child if they are unable to see and assess a child in person, as well as their ability to have a meaningful conversation about immunisations.
Staff training
Crocker-Buque et al (2017) found that 59.7% of overall vaccination-related activity was administrative and described a significant variation between which of this was completed by clinical and non-clinical staff, with some GP practices placing a higher time pressure on administration for nurses. Despite administration being one of the more significant elements of the programme, they state that administrative recommendations are less specific than clinical recommendations and the likelihood of them being implemented is reduced as a result (Grol et al, 1998). Interestingly, training, support and guidance tend to be more robust for the clinical elements of the childhood vaccination programme as nurses undertake annual training, yet there is no equivalent guidance for the non-clinical components to the programme for administrative staff, despite them having a patient facing role and the fact that changes made to vaccine schedules as per The Green Book and vaccine update emails from Public Health England will affect the administrative elements of the programme, as well as clinical (UKHSA, 2020; 2021b). NICE (2009) specifies that all staff involved in immunisation are appropriately trained, though it is unclear whether the reference to ‘staff’ includes non-clinical (administrative) staff. NHS England and NHS Improvement (2019) support the need for access to consistent education, information and support for all roles involved in vaccination (Crocker-Buque et al, 2017) through the use of huddles to disseminate the latest guidance and discuss any issues. McGeown et al (2018) deemed this crucial to improving childhood immunisation uptake. Administrative roles are significant to the delivery of the childhood immunisation programme and NHS England and NHS Improvement (2019) recommend that staffing is expanded within GP practices in relation to practice nurses and support staff, to ‘reduce the burden’ and streamline the delivery of vaccination programmes. Crocker-Buque et al (2017) agree and state that administrative activities involved in vaccination programmes are highly adaptive, as evidenced by the different structures used by different GP practices, and so recommend that tasks are allocated to health care assistants or administrative staff to free up clinical capacity. In contrast, Edelstein et al (2020) and Bedford and Elliman (2020) advised that healthcare practitioners should remain equipped to signpost or address parental concerns.
Immunisation leads
Seven outstanding GP practices within a study completed by McGeown et al (2018) assigned designated staff as immunisation ‘leads’, who were accountable to the Practice Manager in relation to vaccination uptake. This supports the NICE (2009) recommendation for a healthcare professional to be identified in every GP practice to be responsible and provide leadership for the national childhood immunisation programme, ensuring that all staff involved have access to The Green Book and that services are adapted in accordance with updates provided around the Childhood Immunisation Programme. McGeown et al (2018) acknowledge that there is great variation in how the programme is delivered by GP practices across England and although expectations are listed in service specifications, there are no clear mechanisms as to how it should be delivered or monitored. Crocker-Buque et al (2017) recommended that GP practices compare their delivery models with others to determine whether an alternative or adapted model of immunisation programme delivery may be more efficient.
Coordination
IT systems
A missed opportunity for vaccination (MOV) is defined as an occasion when a child, who is eligible for or outstanding a vaccination and has no contraindication to vaccination, attends a health service and does not receive any of the recommended vaccines (Sridhar et al, 2014). An opportunity may be missed when a child attends for treatment of an episode of illness and the WHO (2022) published a strategy to assess and reduce MOVs in health facilities across the world as eliminating MOVs will increase overall immunisation coverage, particularly in those from lower socioeconomic backgrounds (Jacob and Coetzee, 2015). Guidelines can be embedded in IT systems to ensure that clinicians are automatically prompted to vaccinate their patients during contacts (McGeown et al, 2018) and they can also be used to ‘look ahead’ to when a child is next due immunisations (McGeown et al, 2018). Crocker-Buque et al (2017) supported this initiative and suggested that the use of patient tracking or provider prompts to reduce these missed opportunities for vaccination could increase coverage without requiring a significant increase in staff and appointment capacity. Furthermore, Rodewald et al (1999) highlighted that these interventions are more effective when they are used concurrently, rather than in isolation.
The National Audit Office (NAO, 2019) concluded that health system barriers and data system accuracy, as opposed to anti vaccination messages, were the underlying cause of a decline in vaccine coverage. Although time consuming, this increased the accuracy and reliability of practice vaccine data, which corroborates NICE (2009) guidance in relation to ensuring accurate records and effective IT systems to help practices identify and contact children who may not be fully vaccinated, is integral to implementing the vaccination programme successfully. NHS England and NHS Improvement (2019) identified challenges associated with the inputting and sharing of vaccination data between primary and secondary care, and as a result, ensuring that data relating to GP practice performance concerning key immunisation targets is up to date.
Vaccination appointments
Crocker-Buque et al (2017) and Edelstein et al (2020) propose that childhood vaccine coverage can be increased by offering a higher capacity of appointments per child, though it could be argued that increasing the availability of appointments may not be possible for busy GP practices, particularly for those with relatively deprived populations with high need. Without proportionate increases in funding (Kennedy et al, 2011c; Baird et al, 2016) and staffing. As NHS staff shortages included 39 652 nurses and 8 158 doctors as of December 2021 (Campbell, 2022), further research is needed to affirm the accuracy of this claim.
Bedford and Elliman (2020) stated that offering flexible and accessible vaccination services for busy families is vital to improving childhood immunisation uptake, which supports the NICE (2009) recommendation that access to immunisation services is improved by extending clinic times and ensuring they are family-friendly. For example, a GP practice involved in McGeown et al's (2018) study held a catch-up ‘open day’ for childhood immunisations, which involved team members dressing up as cartoon characters and painting activities being held in the waiting room. The event was published to parents in advance, was a fun event and provided the opportunity to engage with parents around other child health issues.
Despite NICE (2009) guidance recommending that there are sufficient vaccination appointments available for children to receive the recommended vaccines on time, Bell et al (2020) reported that parents are experiencing difficulties in booking vaccination appointments for their children. NHS England and NHS Improvement (2019) stated that the accessibility and convenience of appointments is key to increasing vaccination uptake. Nevertheless, challenges remain around the capacity of primary and secondary care services to provide the gold standard of care as, despite a rise in demand, GP numbers have decreased between 2015 and 2019 (Trade Union Congress, 2019) and previous difficulties have been compounded by the current pressures of COVID-19 on the demands for NHS care (Karjalainen, 2021).
McGeown et al (2018) found that providing patients with the ability to book appointments online, increased the number of immunisation appointment bookings. Longer appointment times for patients who do not speak English or who have complex care needs was also considered important (McGeown et al, 2018).
Vaccination delivery sites
Despite the current pressures, NHS England and NHS Improvement (2019) perceived GP practices as delivering high quality vaccinations services and proposed that general practice-led vaccination should remain the main delivery route for most vaccination (Paterson et al, 2018; Christensen et al, 2020). Still, coverage for vaccinations delivered in schools is increasing (Edelstein et al, 2020) and a number of studies have concluded that overall vaccination rates were highest and more equal between two age groups when delivered as part of school-based programmes, compared to GP and pharmacy-based provision. Schools are identified as a desirable place for children to be vaccinated by parents (Paterson et al, 2018; Christensen et al, 2020). Interestingly, despite the socioeconomic gradient in vaccine uptake, Christensen et al (2020) found that on average, vaccine uptake was higher in school-based programmes in the most deprived areas than uptake in GP programmes in the most affluent areas. Paterson et al (2018) anticipated this result and found that parents preferred school vaccination due to the emotional and sometimes anxiety-provoking challenges associated with GP surgeries; they further state that more research is needed to investigate children's anxiety during vaccinations in school, when their parent isn't present as literature states that early vaccination experiences can lead to subsequent vaccine hesitancy (Pebody et al, 2015).
Many school-based immunisation programmes require the completion and return of consent forms by parents in order for the child to be vaccinated. Areas of higher deprivation are associated with low numbers of consent forms being returned and thus children being vaccinated. Barriers such as poor literacy of parents or disorganised ‘book bags’ may contribute. It may be presumed that the non-return of a consent form equates to a family not consenting to vaccination, though this is not the case and children may bypass their right to vaccination through avoidable clerical and administrative failings. The return of consent forms is vital to ensuring the best vaccine uptake rates in schools and this can be enhanced by utilising support methods which are appropriate to the population (Sealey, 2017). Christensen et al (2020) promote the use of vaccine delivery initiatives that reflect the local community, for example, a school within a deprived area began distributing consent forms to parents and carers at the school gates and the rates of return of consent forms and vaccine uptake subsequently drastically increased, as well as each child's opportunity for vaccination.
Family-centred care
Deprivation
Inequalities in vaccination coverage exist globally, as well as nationally as a result of immunisation programmes not providing adequate and accessible services to all communities (Coupland et al, 2007; Hawker et al, 2007; Hutt and Gilmour, 2010; Baker et al, 2011).
Christensen et al (2020) noted a decline in vaccine uptake associated with increased levels of deprivation across all vaccine providers. This claim is supported by Wicker and Maltezou (2014), The NAO (2019) and Crocker-Buque et al (2017), who agree that inequalities in access to healthcare services for some populations, particularly those living in low income urban environments, cause disparities in vaccine coverage. Edelstein et al (2020) noted a recent overall decline in vaccine coverage, which they believe is affected by changing migration patterns and a higher proportion of the population containing groups who face barriers to immunisation (Bell et al, 2019). Hendrix et al (2014) state that health promotion messages that personalise an intervention are likely to be more effective than altruistic public health messages which discuss the ‘needs of the many’ and herd immunity around immunisation.
Despite expectations listed within both the service specification and quality standards in relation to GP practices that implement systems to identify and reduce disparities between local population groups, there is no clear mechanism for this to be delivered or monitored. NHS England and PHE fail to utilise a consistent national approach to engage underserved communities (populations who face barriers in accessing and using services, including those underserved because of geographic location, religion, sexual orientation, gender identity, underserved racial and ethnic populations, populations underserved because of specific needs (e.g. language barriers, disabilities or alienage status) to improve vaccination uptake. One small study found that no GP practices within a pool of nine had services to improve vaccination uptake in such groups, nor the ability to identify them (NAO, 2019). Practices are unable to access data in sufficient detail to be able to assess local inequalities, and often do not have sufficient capacity to design and deliver bespoke interventions. This is despite good evidence for escalating reminder recall activities and alternative models, such as home visiting (Crocker-Buque et al, 2017). Local, regional and national public health teams are responsible and best-placed for identifying disparities, suggesting evidence-based approaches to addressing these and working with GPs to implement such strategies with underserved communities. However, data sharing is now more complex, and the role of regional managers has changed, reducing their ability to support and evaluate GP practices' approaches and strategies further (Chantler et al, 2016).
Culture
Santorelli et al (2020) observed that vaccine uptake is influenced by family ethnicity, socio-economic environment and maternal country of birth (Buelow and van Hook, 2008; Van Lier et al, 2014). ‘Underserved’ populations are defined in the NAO's report as those ‘communities who do not access healthcare in the usual ways’ and therefore can have lower vaccination uptake, such as ‘travellers, recent migrants and some religious faiths’ (NAO, 2019:32). PHE (2019) states that the main barrier to vaccination is that access to vaccination services often does not meet the needs of the local community, a particular problem for larger, traveller, migrant families or those with health problems. Holmström (2021) agree and states that hesitancy can lead to alienation if parents cannot easily access vaccinations. They state that current health education and vaccine service delivery is not effective for all families, particularly for those from cultural and ethnic backgrounds, who require targeted interventions to improve vaccine uptake. NICE (2009) advocate tailoring information, advice and support to parents to ensure they are made aware of the risks and benefits of the childhood vaccinations, which they state should be provided in different formats (e.g. in a parent's first language if they do not speak English). The Celebration Card evaluated by Lwembe et al (2016) sent birthday celebration cards (containing information about upcoming or outstanding vaccinations) to families in a number of different languages in an attempt to support cultural inclusivity, though failed to address more complex and specific issues relating to disparities in coverage between ethnicities. For example, smaller, less well-established ethnic groups require specific targeting to ensure vaccination and appropriate record keeping, as well as children who are not registered with a GP (Wagner et al, 2014). The COVID-19 pandemic and consequential restrictions and lockdowns has disrupted childhood immunisation schedules across the world and the COVID-19 vaccine appears to have negatively affected parents' perceptions of the effectiveness of childhood vaccines (Bedford and Donovan, 2022).
Patient experience
Crocker-Buque et al (2017) did not assess patient experience as part of their review of the implementation of the National Childhood Immunisation Programme across GP practices rated ‘outstanding’ but noted that one of the practices with a low score for the Friends and Family Test (FFT) also had a very poor uptake for adult vaccinations (56.1%), suggesting that quality and patient experience may be linked to vaccine coverage. However, this is only one example and the validity, appropriateness, and amount (lack) of scientific evidence available to support the use of the FFT has been questioned (Davis and Panagiotopoulou, 2014). Yet, Edelestein et al (2020) advocate that the monitoring and understanding of parental views and needs is crucial to ensuring vaccine coverage does not reduce any further.
Communication
Vaccination information
Anti-vaccination messages and vaccine hesitancy among a small minority of patients have been identified as factors which affect childhood vaccination uptake (Rough, 2021). The decline in vaccine coverage in England is of concern, Edelstein et al (2020) attempted to determine whether anti-vaccination sentiment was the likely cause of a decline in childhood vaccine coverage. Contrary to expectation, their analysis implied that anti-vaccination is unlikely to be a major contributor to this. Anti-vaccination messages have been found to be overshadowed by pro-vaccination messages and anti-vaccination messages have actually decreased since 2014 (Gunaratne et al, 2019; Hoffman et al, 2019), which has resulted in anti-vaccination information remaining within anti-vaccination groups (Schmidt et al, 2018). Edelstein et al's (2020) findings are supported by the NAO (2019), though it is believed that anti-vaccination messages on social media do affect the uptake of vaccinations elsewhere in the world, so NHS England is alert to the potential impact of these messages and are emphasising the positive case for vaccination as a result (NAO, 2019).
NICE (2009) published quality standards for aspects of the delivery of the childhood vaccination programme, though it is not centrally known how different GP practices implement the vaccination programme, or whether such standards are adhered to. Lwembe et al (2016) highlighted the lack of information that parents and carers have or are given to make informed decisions about vaccinating their child. Naturally, data implies that a substantial proportion of the public admits a lack of knowledge around vaccines but is open to new information, which should be provided by healthcare providers in order to boost vaccine uptake.
Smith et al (2017) indicated that factors strongly negatively influencing a parent's decision to vaccinate their child included their perceptions about the vaccine being unsafe, causing short-term side effects, long-term health problems or ‘overloading the immune system’. In order to increase a parent's willingness for their child to be vaccinated, it is recommended that communication emphasises the safety and effectiveness of the vaccines, while highlighting a child's susceptibility or risk to developing complications (Sealey, 2017). Smith et al (2017) advise that messages to parents are targeted at those strongly associated with side effects and adverse effects and those amenable to change. Further research is needed on how best to communicate this to ensure the information is clear and factual, while understandable by all parents and carers, of varying reading abilities (Smith et al, 2017).
Working together
Many GP practices reported that the use of a multi-disciplinary approach supports them to maintain good childhood vaccination uptake (McGeown et al, 2018). They perceive the role of the health visitor to be key to improving vaccination uptake as they readily visit parents at home and address vaccine hesitancy and consequently some GPs highlighted the value of working alongside Health Visitors and holding meetings to discuss safeguarding concerns, including vaccine refusal. NICE (2009) guidance recommends that Health Visitors check the immunisations of children up to 5 years, when they join nursery and when they start school, though under the current staffing pressures, many would question the feasibility of this as health visitors aren't generally informed when each child starts nursery. Furthermore, this review would not take place at an age where a mandated contact is due, question how this information would be used part of a holistic assessment, while minimising the effect on staffing capacity.
Crocker-Buque et al (2017) acknowledge variation, in relation to staffing structure and task allocation, in the delivery of the childhood vaccination programme between GP practices. They advocate that this information is distributed to all practices in order for them to compare their existing model of delivery and identify any areas in which it can be made more efficient, particularly in relation to appointment length a this was found to have no impact on vaccine coverage. Some GP practices set up competitions with prizes between one another in relation to vaccination uptake (McGeown et al, 2018). NHS England and NHS Improvement (2019) support this in advocating that GP practices would welcome timely and accurate data sharing around their performance, in order for them to see their contribution to local targets more easily and determine whether it could be made more efficient (Crocker-Buque et al, 2017).
Evidence shows that if patients are able to have an adequate discussion about safety and rationale for vaccines with a healthcare professional, they are more likely to accept vaccinations (Leask et al, 2012; Healy et al, 2015). As part of this, Sealey (2017) advocate effective partnership working between schools and immunisation teams to ensure a smooth and supportive process, which is likely to reassure parents and their children.
Recommendations
Table 4 provides an overview of recommendations for future practice, policy and research.
Table 4. Recommendations for future practice, policy and research
| Theme 1. Reminder and recall Text message remindersCall and recallEscalating remindersCatch up programmesInnovations | Patient reminder and recall systems are a crucial mechanism to improving immunisation uptake, yet variation exists in how these are utilised by GP practices across England (Crocker-Buque et al, 2017). |
| NICE (2009) recommends that tailored invitations are sent for immunisations and escalated to invitation via telephone if a child is not brought or a family isn't contactable, taking into account a family's first language and literacy levels and using interpreters or alternative forms of contacts to support this accordingly. | |
| Childhood immunisation uptake is generally lower among families of BAME and low income groups (Forster et al, 2017) and additional targeted campaigns are needed for these groups as a result (Bell et al, 2020) as they are often underrepresented in vaccination services, alongside those not registered with a GP. Further analysis is needed outside of this review (which focuses on the population as a whole) to explore which targeted interventions would promote improved childhood immunisation uptake in different population groups | |
| Understanding how to provide services and improve vaccine coverage for patients who frequently do not attend is identified as an opportunity for further research (Crocker-Buque et al, 2017). | |
| Innovative and creative initiatives such as Celebration Cards to remind parents of their child's upcoming or outstanding immunisations, as well as family fun day ‘catch-up open days’ which provide a positive and accessible place for children to become up to date with their childhood vaccinations (Lwembe et al, 2016; McGeown et al, 2018) have been found to be highly effective through qualitative data collection and analysis. Further research is needed to fully quantitatively evaluate their effect on childhood vaccine uptake, which will be challenging, given the number of other uncontrollable factors that influence uptake. | |
| Theme 2. Healthcare Professionals and staff Immunisation leadsStaff rolesStaff training | Evidence stipulates that parents are more likely to accept vaccinations if they are able to have an adequate discussion about the safety and rationale for vaccines with a healthcare professional, who must be able to address parental concerns with confidence (Edelstein et al, 2020) and the national shortage of health visitors has influenced the decline in childhood immunisation uptake (Wilkinson, 2022). Scotland's vaccine uptake has in fact increased and suggests that their increased number of health visiting mandated contacts has supported this. The utilisation of skill mix staff, such as health care assistants in some aspects of the childhood immunisation programme is recommended by NHS England and NHS Improvement (2019), as well as Crocker-Buque et al. (2017) to increase the capacity of registered staff and the opportunities to utilise innovations to improve vaccination uptake. The use of skill mix staff is also key within Health Visiting services and is recommended by PHE (2021b) to support current pressures, though it should be ensured that skill mix staff members are appropriately educated and prepared. Hounslow and Richmond Community Healthcare Trust piloted using staff nurses, in place of registered health visitors, to complete antenatal and new birth visits and achieved positive outcomes in relation to targets and patient experience (HSJ, 2018). Further research is needed to examine whether and which skill mix might be suitable to support the promotion of immunisations alongside health visitors during the national shortage. It would also be valuable for services to review their policies or standard operating procedures in relation to what discussions are held during mandated contacts and any potential variation between what different practitioners may offer. |
| It is recommended by NHS England and NHS Improvement (2019) that all staff involved in immunisations have access to appropriate education, information, and support. This training and support, such as using regular huddles to disseminate the latest guidance and to discuss any issues, should be extended to all staff involved in childhood immunisations to improve service delivery, as well as staff development. Similarly, NHS England and NHS Improvement (2019) recommend that staffing is expanded within GP practices in relation to practice nurses and support staff, to ‘reduce the burden’ and streamline the delivery of vaccination programmes. | |
| NICE (2009) recommend that a healthcare professional is identified in every GP practice as an ‘immunisation lead’, accountable to the practice manager in relation to vaccination uptake. Crocker-Buque et al. (2017) recommend that GP practices compare their delivery models with others to determine whether an alternative or adapted model of immunisation programme delivery may be more efficient, and NHS England and NHS Improvement (2019) encourage the timely sharing of data with GP practices to enable them to benchmark their performance and contribution to local targets. | |
| Theme 3. Coordination Vaccination appointmentsIT systemsVaccination delivery sites | Challenges exist in ensuring that vaccination data is up to date and flows between pharmacies, secondary care and general practice. The known system issues which prevent efficient vaccine delivery need to be addressed, planning ahead, maintaining accurate patient records are all crucial to improving vaccination uptake in general practice (McGeown et al, 2018). Edelstein et al. (2020) recommend a coordinated approach to commissioning, implementing, delivering, monitoring and governing the childhood immunisation schedule, with clear roles and responsibilities in order to identify and address the causes of the decline in vaccine coverage. |
| The accessibility, convenience and availability of childhood immunisation appointments is key to improving the uptake of childhood immunisations (NHS England and NHS Improvement, 2019). Providing the opportunity for families to book appointments online is likely to increase appointment bookings (McGeown et al, 2018), though consideration should be given to families for whom barriers to accessing appointments may exist, such as those who do not speak English. Such online booking systems may provide an opportunity for translation or read aloud (for families with limited reading abilities) software to be embedded and to remove such barriers. | |
| A number of studies have concluded that overall vaccination rates were highest and more equal between two age groups when delivered as part of school-based programmes, compared to GP and pharmacy-based provision. despite the socioeconomic gradient in vaccine uptake, Christensen et al. (2020) found that on average, vaccine uptake was higher in school-based programmes in the most deprived areas than uptake in GP programmes in the most affluent areas and schools are identified as a desirable place for children to be vaccinated by parents (Paterson et al, 2018; Christensen et al, 2020). | |
| Further research is needed to establish whether or not this would also be feasible within early years settings, such as nurseries and how this improved uptake as a result can be replicated for those not in education settings or those under 1 year, as well as around the anxiety of children being vaccinated in school without a parent present (Paterson et al, 2018). When immunisations are delivered in schools, additional information provided via a poster or parent talk should be provided in order to support the principle of informed consent when a meaningful conversation with a healthcare professional is not available (Sealey, 2017). | |
| Theme 4. Family-centred care CultureDeprivationPatient experience | Poor vaccination uptake is associated with increased levels of deprivation (Christensen et al, 2020). Health promotion messages that personalise an intervention are likely to be more effective than altruistic public health messages which discuss the ‘needs of the many’ and herd immunity around immunisation (Krisitin et al, 2014). Further research is needed to examine the role of public health teams in identify local inequalities and supporting GP practices to design and deliver bespoke interventions for their community. |
| Vaccine uptake is influenced by family ethnicity, socio-economic environment and maternal country of birth (Buelow and van Hook, 2008; Van Lier et al, 2014). Some communities and population groups access healthcare services differently and may have lower vaccine uptake than others (NAO, 2019). Current health education and vaccine service delivery is not effective for all families and targeted interventions are needed to reduce vaccine hesitancy, potential alienation from healthcare services and improve uptake. The COVID-19 pandemic and consequential restrictions and lockdowns has disrupted childhood immunisation schedules across the world and the Covid-19 vaccine appears to have negatively affected parents' perceptions of the effectiveness of childhood vaccines (Bedford and Donovan, 2022). Further research on why vaccine uptake rates have reduced following Covid-19 and whether this demonstrates causality in relation to vaccine fatigue or vaccine hesitancy, as well as education that not all vaccines work in the same way is required. It is recommended that prompt and sustained communication is provided by GPs and national Public Health bodies to raise awareness about the continuation and importance of timely vaccination, as well as the measures implemented to reduce disease transmission in GP practices to promote childhood vaccination uptake during a future pandemic. | |
| Crocker-Buque et al (2017) and Edelstein et al. (2020) perceive parental views to be crucial to ensuring vaccine coverage does not diminish any further. Further research is needed to investigate the link between patient experience and childhood vaccination uptake. | |
| Theme 5. Communication Immunisation informationWorking together | Anti-vaccination messages tend to be contained with anti-vaccination groups in the UK and so far, have not been linked to causing the decline in childhood immunisation uptake (Schmidt et al, 2018; Edelstein et al, 2020). Anti-vaccination messages on social media do affect the uptake of vaccinations elsewhere in the world, so it is important to be alert to the potential impact of these messages and ensure that practitioners emphasise the positive case for vaccination as a result. |
| Anti-vaccination messages tend to be contained with anti-vaccination groups in the UK and so far, have not been linked by causing the decline in childhood immunisation uptake (Schmidt et al, 2018; Edelstein et al, 2020). Anti-vaccination messages on social media do affect the uptake of vaccinations elsewhere in the world, so it is important to be alert to the potential impact of these messages and ensure that practitioners emphasise the positive case for vaccination as a result. | |
| A substantial proportion of the public admits a lack of knowledge around vaccines but is open to new information and more likely to accept vaccination if such information is provided by a healthcare provider. Smith et al. (2017) advise that messages to parents are targeted at those strongly associated with side effects and adverse effects and those amenable to change. It is recommended that communication emphasises the safety and effectiveness of the vaccines, while highlighting a child's susceptibility or risk to developing complications. Further research is needed on how best to communicate this to ensure the information is clear and factual, while understandable by all parents and carers (Smith et al, 2017). | |
| Many GP practices perceive multi-disciplinary working to be key to improving childhood immunisation uptake (McGeown et al, 2018), though capacity challenges within both health visiting services and GP Practices threaten the quality. Further research could provide insight into how GPs and Health Visiting Service could work together most efficiently, given the capacity challenges. | |
| Crocker-Buque et al (2017) and NHS England and NHS Improvement (2019) suggested that GP practices would welcome timely and accurate data sharing around their performance, in order for them to see their contribution to local targets more easily and determine whether it could be made more efficient (Crocker-Buque et al, 2017). | |
| GP practices report access to clinical commissioning groups' immunisation leads to be supportive in providing expertise around immunisation (McGeown et al, 2018). |
Limitations
Studies which explore how child immunisation uptake could be improved in specific patient groups were excluded from this review for pragmatic reasons, meaning that some potential factors that could be relevant to a general population could have been overlooked. Results were not limited to individual vaccines and it may be that uptake is improved differently for different vaccines, which are given in different locations and at different stages in a child's life. Differing strengths of association between factors which improve uptake and specific vaccines may exist.
Literature not published in English were excluded due to time and cost constraints and only one person carried out the literature search, analysis and systematic review so the risk of human error or experimenter bias cannot be eliminated.
Conclusions
This systematic review has explored how the uptake of childhood immunisations can be increased in England. The findings of this review highlight the high value and cost effectiveness of reminder and recall systems in improving childhood vaccination uptake, but that tailored and innovative interventions should be used as well as this in order to improve the uptake of underserved populations who may experience barriers to accessing healthcare services (Bell et al, 2018). Current health education and vaccine service delivery is not effective for all families (Holmström, 2021) and targeted interventions are needed to improve this, such as innovations, gaining an understanding of an individual family's needs, literacy and language levels, and utilising interpreters or alternative communication support mechanisms as indicated (NICE, 2009). IT systems require review and should be kept up to date to ensure that patient tracking and prompts work effectively. Meaningful conversations about childhood vaccinations should be encouraged at every healthcare contact and, following an informed choice and consent, a catch-up plan generated, or vaccination given opportunistically (Kraszewski, 2017) to support improved childhood immunisation uptake.
Moreover, staffing structures within GP practices heavily influence the efficiency of the delivery of the childhood immunisation programme and vaccination uptake. The findings within this review recommend that staffing structures are reviewed in order to free up registered staff and clinical capacity and support improved access to immunisation services and appointments, which are family-friendly (Crocker-Buque et al, 2017). Effective therapeutic relationships that are built with parents, carers and children by healthcare professionals promote positive vaccination experiences and improved vaccination uptake as a result.
Additionally, access to training, education and regular support for all staff, including administrative roles, is crucial to the safe and effective delivery of childhood immunisation programmes and should be ensured (McGeown et al, 2018). Schools are considered a desirable place for school-aged children to be vaccinated and one which promotes equal vaccination uptake between deprived and affluent communities (Christensen et al, 2020). The value of multidisciplinary working and ensuring a coordinated approach to the delivery of vaccination programmes have also been highlighted as key factors to improving childhood immunisation uptake within this review.
Some links have been made between poor patient experience and poor vaccine uptake (Crocker-Buque et al, 2017). Patient experience influences decision-making and, hence, it is vital that GP practices monitor patient experience, understand patient views and make changes to service delivery to support this where possible to ensure that childhood vaccination uptake does not reduce any further. It is not believed that anti-vaccination messages contribute to the reduced childhood vaccination coverage in the UK (although this could have changed as a result of the COVID pandemic), yet it is understood that anti-vaccination messages on social media do affect uptake of vaccinations elsewhere in the world so practitioners should remain alert to the potential impact of anti-vaccination messages circulating worldwide, particularly on social media, and continue to emphasise positive, evidence-based reasons for vaccination (NAO, 2019).