

Although most Swedish school children state that they have good social relationships, relatively few health problems and a high level of wellbeing, perceived school stress is increasing, especially among adolescents (László et al, 2019). Physical activity remains low, and more children and adolescents report symptoms such as headaches, stomach-aches, anxiety, depression and sleeping problems related to the use of digital media (Patton et al, 2018). Moreover, problematic relationships with friends, family and difficulties coping with schoolwork may also have an impact on young people's wellbeing (Wickström and Lindholm Kvist, 2020). Health promotion efforts directed toward this group are key to supporting them in everyday life. The school health service (SHS) in Sweden where school nurses and school physicians work, is a unique platform for providing legally required health activities (Levinson et al, 2019). The distribution of resources is different for school nurses and school physicians. School nurses are the key persons within the SHS and meet virtually all children continuously during their school time. The presence of a school physician varies significantly between different municipalities depending on resource allocation. In many municipalities most school children do not meet the school physician during the school years because the availability of school physicians is only sufficient for consultation for medical or health related difficulties in school. The Swedish government suggests limiting the number of school children to 430 per school nurse and 7 000 per school physician. Furthermore, the SHS's resources should also be allocated for existing goals and health promoting activities and not only according to the number of school children (National Association for School Nurses, 2022). The basic health programme for key ages includes promotion and prevention work and spontaneous and follow-up visits. All school children, regardless of age, have access to the SHS and there are several opportunities during a school period to build relationships between school children, school nurses and school physicians (Morberg, 2012). The prerequisite is, of course, that the school children have trust in the SHS provided. Professionals within the SHS base their work on the United Nations Convention on the Rights of the Child, which was written into Swedish law on 1 January 2020 (Regeringskansliet, 2018). The law states that all actions undertaken by public and private institutions must assure the best interest of the child, and that the child's views and rights to express those shall be a primary consideration. One way to follow the law is by inviting school children to participate in their own care and ask for school children's views of care (Gurung et al, 2020).
Aims
To reach a high-quality standard of care, investigations of the SHS should be made on a regular basis (Levinson et al, 2019). In Sweden, there is no evaluated questionnaire to measure school children's perception of the SHS. Measurement of quality of care should address the complexities in the construct. The Institute of Medicine suggests that efforts to improve health care quality should be focused on six areas: effectiveness, efficiency, equity, person centredness, safety, and timeliness (Hibbard et al, 2004). Sweden has identified these areas as prerequisites for achieving quality in health care and as the basis for systematic quality improvement (National Board of Health and Welfare, 2009). The National Patient Survey (NPS), which is a recurrent national survey of patients' experiences of health care has been conducted since 2009 and aims to collect and compare results of experiences of care from all parts of the country. However, it is perceptions of quality, rather than clinical indicators of quality, which should drive service utilisation (Hanefeld et al, 2017). An important point of quality improvement is to ask users how they experience the services. For instance, school children cite the importance of accessibility to the SHS and the possibility of spontaneous visits (Kivimäki et al, 2019). One way to study school children's views and to allow school children to participate when building a set of measurable indicators based on school children's perspective (Kivimäki et al, 2019; Gurung et al, 2020) is to develop a questionnaire that takes its starting point from the quality indicators mentioned earlier. The purpose of this pilot study was two-fold. First to develop a set of questions to measure experience and satisfaction of the services provided by the SHS, second to perform initial testing of two age-matched questionnaires for SHS. Our research questions were:
- What is the acceptance and applicability of the questionnaires?
- How do school children describe experience and satisfaction of the care in the SHS?
- Are there any differences between younger and older age-groups?
Methods
This is a cross-sectional descriptive pilot study in two steps including development and testing of two age-matched 11 item-comprehensive questionnaires, addressed to younger school children (6–12 years) in compulsory school and to older school children (13–18 years) in compulsory school and upper secondary school.
First step: questionnaire development
We started with the specific dimensions used in the Swedish National Patient Survey. These are information, participation, accessibility, continuity, respect, emotional support, and overall impression. Each dimension consists of several items linked to health care. In order to adjust the items to fit the SHS, a guide for each dimension was created and a draft of items was presented for an expert panel who assisted in the development. The panel consisted of school nurses (n=4), school physicians (n=2) and representatives for the student organisations (n=2). Recruitment of participants to this group was initiated from the national quality register of the SHS. The questionnaire was developed to account for school children having met both the school nurse and the school physician. Hence several items require the respondent to consider the school nurse and the school physician in the same item. In addition to demographic data, the items had a response scale on a nominal scale for three items (1–2), and a four-grade ordinal scale for seven items (3–10). A horizontal scale from one (worst imaginable) to ten (best imaginable) was used for the last item (also at ordinal level). The questionnaire for younger children used two smiles (one happy and one sad to correspond to best and worst imaginable) for this item. The authors contacted the head of the SHS in one of the top ten biggest municipalities in Sweden. School nurses working in compulsory and upper secondary schools were asked to invite children to participate in focus groups; two focus groups for each age group. Information letters were sent and consent to participate was obtained. Cognitive interviews (cognitive debriefing) were performed using a think-a-loud method (Meadows, 2021). Interviews were performed in a separate room at three different schools during school time for approximately 30 minutes. Two focus groups for the younger school children (n=10) with mixed genders were included and two focus groups for the older school children (n=15) with mixed genders were included. The interviews were carried out by two authors (CP and YS). Interviews were recorded and notes were written during the session. Before the beginning of the interviews, each child received a copy of the questionnaire and then the interview leader read questions aloud before asking probing questions about how each question was interpreted and what the children were thinking regarding response options. For each item, a set of questions were asked: ‘Do you understand the question?’, ‘Is the question clearly described?’, ‘Is the question important?’, ‘What do you think about the response options’ and ‘Other things to add?’
Second step: sample selection and data collection
After consent from the head of the SHS in a municipality in the southeast of Sweden, an information letter about the purpose of the study was sent to the principals at three schools. Two schools were located in the city, and one in a rural area. For all schools, the number of school children per school nurse was approximately 500. Only school children who had a health visit at the SHS during the past year were included. The school nurse in charge distributed an equivalent information letter to school children and their caregivers through the school's learning platform. Requests asking for consent to participate in the study were sent by post to school children and their caregivers' home address. Before performing data collection, written consent from caregivers was requested for school children. School children in the upper secondary school gave consent themselves. The questionnaires were answered anonymously during school time and were collected by the school nurse in charge.
Data analysis
Data collected in the think-aloud sessions was written during each session by the interviewer and was compiled into a spreadsheet to visualise results from all four focus groups (Eccles and Arsal, 2017). Then, the research group discussed all suggestions until consensus was achieved. Data analysis of collected questionnaires were performed using the Statistical Package for the Social Sciences (SPSS), version 26. Descriptive statistics were used to characterise demographic data. Results are presented in numbers and percentages for each item in the separate questionnaires. Inferential statistics were used to calculate differences between the questionnaires at an item level. If a schoolchild replied that they had ‘not met the school nurse’, they were removed from the analysis (Stockemer, 2018). None of the school children in the pilot study had met the school physician, hence there are no descriptions of school children's experience and satisfaction of the school physician. A chi-square test was used, and the significance was accepted at the level of p<0.05.
Ethical approval
The Regional Ethical Review Board in Linköping, Sweden (Dnr 2017/480-31) formally approved the study. The principals, school nurses and the head of the SHS were given written information about the aim of the study. School children and caregivers were given written and oral information about the aim of the study and that the participants had the right to withdraw from the study at any time (Helgesson, 2015).
Results
First, we describe the results when developing the questionnaires using the expert panel and the think-a-loud technique, then follows a description of experience and satisfaction described from the results of the questionnaires and a comparison between the younger and older age group.
Acceptance and applicability of the questionnaires
To describe acceptance, face validity was investigated by discussions with members in the expert panel to determine whether the two questionnaires covered the most important items within the dimensions described in the NPS. The group reached consensus about following the same dimensions as the questionnaires for the health-care sector but reducing the number of items. This resulted in adapted questionnaires with 11 items distributed within the seven dimensions: information (2), participation (2), accessibility (3), continuity (1), respect (1), emotional support (1) and overall impression (1). Thereafter, cognitive interviews were performed to investigate applicability. Suggestions from school children led to the revision of the wording of the questions to improve readability and to reduce ambiguity. School children suggested changes in item numbers 4, 7 and 8. They also wanted numbers written out on the scale in the last item, but they deemed all items important to describe their experiences of visiting the SHS. The older age group suggested a clarification in item number 10 and that the alternative ‘not met the school nurse’, was added in item number 11. This was described as important because school children sometimes made a choice to visit the Youth Guidance Centre (which is a separate service where adolescents can make their own appointments to other health-care professionals) instead of the school nurse, and then the answer to item 11 would be misleading. In conclusion, adjustments in items lead to slightly different wording between the two age-matched questionnaires (Table 1).
Table 1. The results after adjustments according to the cognitive interviews, which led to different wording in five items. The differences between questionnaires are marked in bold text below
| Item | Items in questionnaire | |||
|---|---|---|---|---|
| Younger children (7–12 years) | Older children (>12) | Dimension | Response options | |
| #1 | I know who my school nurse is | I know who my school nurse is | Accessibility | Yes/no |
| #2 | I know where to go whenI want to see the school nurse | I know where to go whenI want to see the school nurse | Accessibility | Yes/no |
| #3 | I feel that I can see the school nurse when I need to | I feel that I can see the school nurse when I need to | Accessibility | Totally agree, partly agree, partly disagree, totally disagree |
| #4 | I feel that they listen to me when I tell things to my school nurse | I feel that they listen to me when I tell things to my school nurse | Respect | Totally agree, partly agree, partly disagree, totally disagree |
| #5 | I feel that they give answer to my questions | I feel that they give answers to my questions | Information | Totally agree, partly agree, partly disagree, totally disagree |
| #6 | They describe to me in a way that I understand | They describe to me in a way that I understand | Information | Totally agree, partly agree, partly disagree, totally disagree |
| #7 | I can talk about things that are important to me, when I see the school nurse | I am involved in decisions about what to talk about when I see the school nurse | Participation | Totally agree, partly agree, partly disagree, totally disagree |
| #8 | I am involved in decisions about what's important to me when I see the school nurse | I participate in decisions about my health when I see the school nurse | Participation | Totally agree, partly agree, partly disagree, totally disagree |
| #9 | I feel comfortable together with the school nurse | I feel comfortable together with the school nurse | Emotional support | Totally agree, partly agree, partly disagree, totally disagree |
| #10 | I receive the support I need from the school nurse if I need to meet with a social worker | I get the help I need to get in contact with others in the school service (social workers, physicians, special teachers, psychologist) | Continuity | Totally agree, partly agree, partly disagree, totally disagree |
| #11 | Overall, what is your opinion about the visit to the school nurse | Overall, what is your opinion about the visit to the school nurse | Overall impression | 1= worst imaginable to 10 = best imaginable |
Description of school children's experience and satisfaction of the SHS
A total of 165 questionnaires were distributed and 141 answers were returned, producing a response rate of 86%, which was deemed satisfactory. Of this number, 55 school children belonging to the younger age group and 86 to the older age group estimated their satisfaction with the SHS (Table 2). The distribution of answers across all dimensions in all items show ceiling effects, with major responses described in total agreement to the statements in the items. According to Chyung et al (2020), ceiling effects can occur when a questionnaire has limitations in its sensitivity, but when measuring experiences as is the case here, it is difficult to accurately measure individual respondent's true responses and distinguish them from other respondents. This results in a low variance in the data. In the analysis, the alternative ‘not applicable’ was removed. Therefore, the number of dropouts increased, especially in the older age group (Table 2).
Table 2. Results from Chi-square analysis
| Younger age group n=55 of 62Girls= 33, Boys= 22 (no answer 7) | Older age group n=86 of 103Girls= 54, Boys=32 (no answer= 17) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| totally agree (yes) | partly agree | partly disagree | disagree (no) | n | totally agree (yes) | partly agree | partly disagree | disagree (no) | n | ||
| Dimension | Item | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Accessibility | 1* | 53 (96) | 2 (4) | 55 | 63 (73) | 23 (27) | 86 | ||||
| 2 | 53 (96) | 2 (4) | 55 | 79 (92) | 9 (8) | 86 | |||||
| 3** | 28 (51) | 24 (44) | 1 (2) | 2 (4) | 55 | 40 (47) | 27 (31) | 13 (15) | 5 (6) | 85 | |
| Respect | 4** | 52 (98) | 0 | 1 (2) | 0 | 53 | 53 (80) | 11 (17) | 3 (5) | 0 | 66 |
| Participation | 7 | 43 (81) | 10 (19) | 0 | 0 | 53 | 45 (69) | 16 (25) | 4 (6) | 0 | 65 |
| 8 | 40 (77) | 8 (15) | 2 (4) | 1 (2) | 52 | 45 (71) | 14 (22) | 4 (6) | 0 | 63 | |
| Information | 5 | 41 (77) | 12 (23) | 0 | 0 | 53 | 47 (72) | 17 (26) | 1 (2) | 0 | 65 |
| 6 | 37 (70) | 16 (30) | 0 | 0 | 53 | 48 (74) | 16 (25) | 1 (1) | 0 | 65 | |
| Emotional support | 9 | 49 (92) | 4 (8) | 0 | 0 | 53 | 53 (80) | 8 (12) | 3 (5) | 2 (3) | 66 |
| Continuity | 10 | 34 (69) | 12 (24) | 1 (2) | 2 (4) | 49 | 32 (68) | 11 (23) | 4 (9) | 0 | 47 |
p<0.05
In the comparison between the age-matched questionnaires using the Chi-square analysis, statistical differences occur in two dimensions (Table 2). Two items in the dimension of accessibility show differences. First, ‘I know who my school nurse is’ shows that more school children in the younger age group answer yes to that question (96%) in comparison to the school children in the older age group (75%) (p<0.000). Secondly, the item ‘I feel that I can see the school nurse when I need to’ also shows where the distribution of answers across the scale varies between the two age groups, and the variation is more scattered in the answers from school children in the older age group (p<0.05). In the dimension of respect, the item ‘I feel that they listen to me when I tell things to my school nurse,’ also shows variations in answers between the age groups, where more school children in the younger age group are more positive than school children in the older age group (p<0.05). The last item concerning overall impression where school children have graded their visit at the SHS on a scale from 1 to 10 is described in Figure 1. Here too, a ceiling effect is apparent: only five school children have estimated lower than five on the scale.
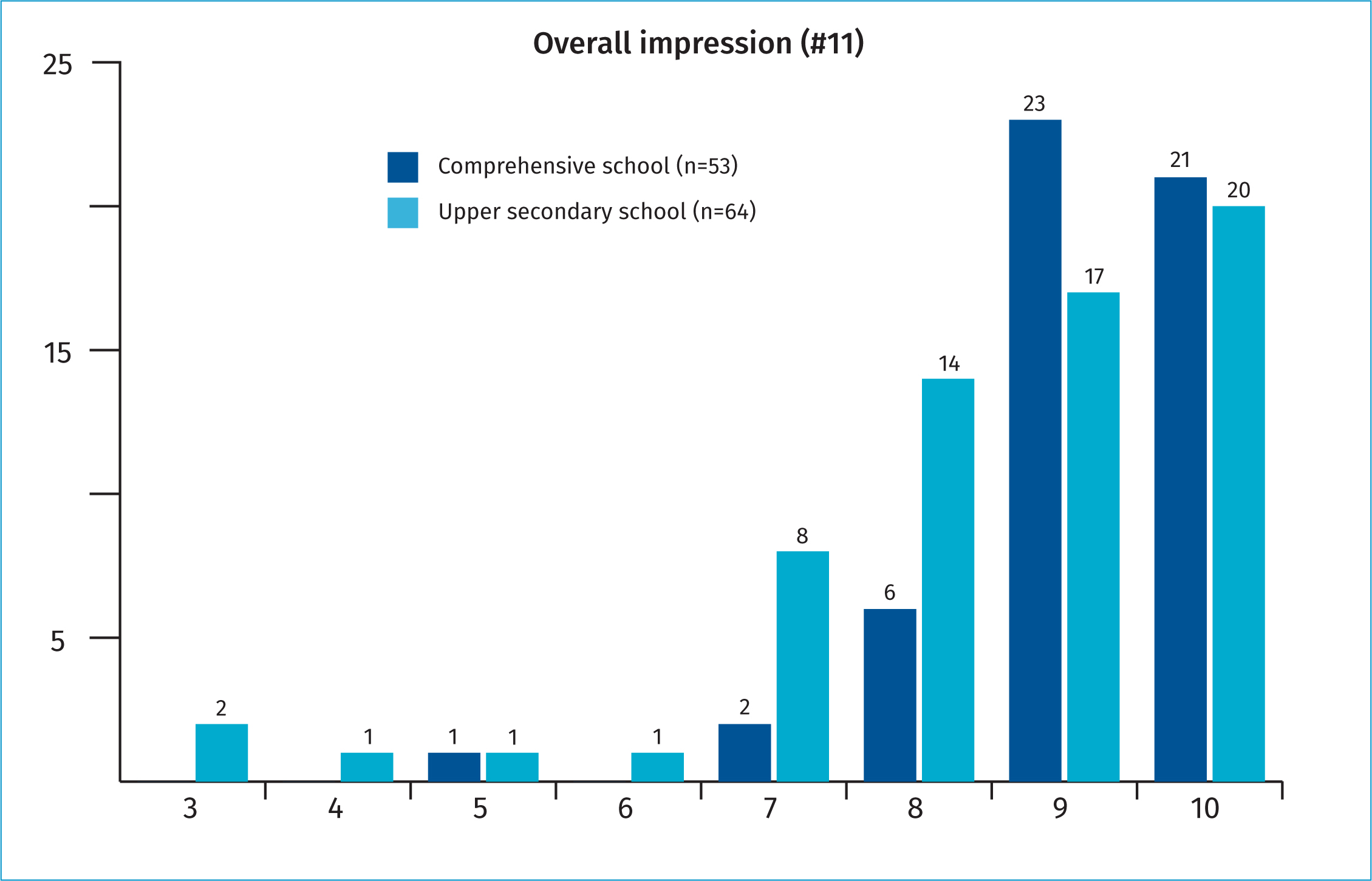
(p<0.05). In the dimension respect, the item about ‘I feel that they listen to me when I tell things to my school nurse’ also shows variations in answers between the age groups, where more school children in the younger age group are more positive than school children in the older age group (p<0.05). The last item describing the overall impression where school children have graded their visit at the SHS on a scale from 1 to 10 are described in Figure 1. Here too, a ceiling effect is apparent: only five school children have estimated lower than five on the scale.
Discussion
To date, there is no known validated questionnaire designed to evaluate the quality of the SHS in Sweden. To improve the SHS, the experiences of school children are valuable. Few studies have addressed this and to our knowledge, this is the first study in Sweden which has developed such a questionnaire for the SHS. The result of this study describes the development and initial testing of the two age-matched questionnaires. School children's views were considered when the questionnaires were designed. The result shows that the questionnaires are acceptable and applicable. Overall, in both the younger and older age groups, school children showed a high level of satisfaction of the SHS. When comparing the questionnaires, there were significant differences in experienced satisfaction between the younger and the older age groups in two of seven dimensions: accessibility and respect. This result should be considered in accordance with the knowledge that child health nurses have a key prominent role during the toddler years as well as during initial schooling, building a trusting relationship with frequent and regular health promotion activities for the whole family (Stenmarker et al, 2021). According to the results of the cognitive interviews for both questionnaires, adjustments were made to render them more applicable. This highlights that the involvement of children from the target group is crucial in such a developmental process (Steinhart et al, 2021).
The accessibility dimension measures whether the school children know who their school nurse is, where the school nurse is located and whether they can visit the school nurse when they need to. Almost all in the younger age group knew who the school nurse was, but a quarter of the older school children did not know. This might be explained by more frequent health visits among younger children required in the basic health program in Sweden. Compared to the younger group, the older age group were less likely to reply that they could visit the school nurse when they needed. Older school children may also need help at short notice, which can be difficult if a school nurse has an excessive workload. A previous study has shown that teenagers turn to other agencies such as the Youth Guidance Centre or seek information via the internet (Smart et al, 2012). It is known that mental health problems are increasing in general among school children and more so as they grow older (Wickström and Lindholm Kvist, 2020). For this reason, the access to support from the school nurse during a school day may be crucial. The school nurse workload must accommodate accessibility for time-consuming health problems such as mental health problems (Ellertsson et al, 2017).
In the dimension of respect, most school children felt that they were treated in a respectful way and were listened to. This is in accordance with the Convention on the Rights of the Child, one of the basic principles that all children have the right to express their opinion and to be respected (United Nations, 2022). There were significant differences between the age groups where the older age group did not agree to the same extent as the younger group of school children. In person-centred nursing, the partnership is based on mutual respect and the fact that the person's story is listened to (Weath et al, 2018; Cronenwett et al, 2007). The result shows school nurses follow this principle when meeting with school children. The relationship between school children and the school nurse is important. To achieve a trusting relationship, school children should feel comfortable asking about issues concerning health problems and be treated with respect (Smart et al, 2012). Does a schoolchild's feeling of confidence for the school nurse diminish with increasing age and are there are other actors they can turn to in order to have their needs met? Previous studies have indicated school nurses' lack of knowledge in essential health areas such as sexual and reproductive health and rights (Aranda et al, 2018; Silivri et al, 2021) and mental health (Jönsson et al, 2019), which are areas that affect older school children. One way to connect with the older school children is to use participatory approaches to identify what they want and what their needs are (Kivimäki et al, 2019). This is a challenge and it requires knowledge and a school nurse workload adapted to accommodate timely and uninterrupted visits.
In the dimension of emotional support, school children describe that they felt comfortable with the school nurse. The younger school children agreed with this to a larger extent than the older school children. Since the older age group states that they cannot meet the school nurse when they need to and do not completely agree that they are listened to, it suggests that it is difficult for them to get the emotional support they would like.
The school children stated that they understood the information provided by the school nurse and that the school nurse answered their questions. This shows that school nurses adapt to the schoolchild's cognitive level and use a person-centred approach (Harder et al, 2017). However, a Swedish study showed that school nurses reported limited Sexual and Reproductive Health and Rights knowledge and sometimes referred students to the Youth Guidance Centre (Silivri et al, 2021). When school nurses are not confident of their knowledge, it impacts what and how they provide information. If referrals to other caregivers are made due to lack of knowledge, an improvement in quality of care provided is needed.
In the dimension of participation, school children estimated how satisfied they were in being involved with making their own decisions regarding health issues. Most of the pupils in both the younger and older age groups felt that they participated, which is in line with the Convention on the Rights of the Child, which states that all children have the right to be involved in issues concerning them and their feelings (Regeringskansliet, 2018). To engage and involve school children to make their own decisions leads to increased self-esteem and thus an increased feeling of having control over the situation (Bombard et al, 2018).
Limitations
One limitation is that an attrition analysis was not possible because the non-responders were unknown to the research group. Another limitation is that the definition of the concept quality of care was grounded in the health-care sector rather than from a health promotion perspective, which is the central commitment in SHS. This may have limited the scope of selected items. The expert panel before selecting items was used to counteract this limitation. The sample size is small for more sophisticated psychometric analysis and the results must be seen considering these limitations. It is also important to highlight another ethical aspect when evaluating this kind of questionnaire. In Sweden it is common that a school nurse works alone and has the responsibility of only one school. Therefore, the evaluation of each SHS unit may be an issue since the answers can relate to the school nurse's work. One suggestion is that the management of the SHS should be aware of this potential problem and reflect on how the results should be presented and discussed when improvement is needed.
Conclusions and implications for the SHS
For several years, health-care providers have requested a national questionnaire in the SHS. This study provides a tool that may be useful to guide improvement efforts. Requesting school children's views can impact these improvement efforts. Involving school children in the quality-of-care process may lead to better services. Future research should include a larger national study with school children from different municipalities and socio-economic backgrounds as well as children with chronic conditions and disabilities. In addition, studies about how the implementation of improvement efforts leads to better results on individual, group and organisational levels would be of interest.
KEY POINTS
- This is the first Swedish study that has developed and tested two age-matched questionnaires which enable school children to express their experiences of the care given by SHS.
- By inviting school children to answer this kind of questionnaire, the professionals and managers will gain more knowledge of school children's experiences of different dimensions of care.
- It is an important task for the SHS to listen to and follow up school children's experiences of the care given and let this have an impact on improvement efforts.
REFLECTIVE QUESTIONS
- What do we know about school children's experiences of the SHS?
- How do the experiences of care differ between younger and older school children?
- How do school children experience the accessibility, respect, information, participation, continuity, emotional support and the overall impression when visiting the SHS?
- How do we use our knowledge of school children's experiences to improve the SHS?
- What did you learn from this study?