


The 2017 British Mental Health of Children and Young People in England (NHS Digital, 2018) found that 1 in 8, 5–19-year-olds had at least one mental disorder; and the Wave 1 and 2 follow-up surveys suggest that mental health difficulties have been exacerbated by the coronavirus pandemic (NHS Digital, 2020; 2021). However, studies have found that fewer than one third of children and young people in need of support receive services (Dvorsky et al, 2014; Newlove-Delgado and Ford, 2020). Failure to address mental health difficulties early in life affects individuals' long-term functioning and wellbeing and may also generate significant societal costs related to increased health care usage, unemployment, and antisocial behaviours (Chief Medical Officer [CMO] 2012; 13).
The UK Government Green Paper on Children and Young People's Mental Health (Department of Health [DH] and Department for Education [DfE], 2017) sets expectations for schools to take a central role in the identification of and response to mental health difficulties (MHD). The DfE has issued non-statutory guidance to schools (DfE, 2018) and since 2018, local areas have been invited by NHS England and Improvement to establish mental health support teams (MHSTs), working with a cohort of local schools and pupils to provide early intervention on some mental health and wellbeing issues.
There is some evidence that systematic, universal school-based screening approaches detect a greater proportion of children and young people with MHD compared with less formal processes (Dvorsky et al, 2014; Anderson et al, 2019; Newlove-Delgado and Ford, 2020) and a goal of universal screening is to identify childhood problems before the behaviours exceed the threshold of a parent or teacher referral for services and to provide a pathway to early intervention services. Despite these reported benefits, there is no nationally defined programme of screening and identification for mental health problems and mental health difficulties in primary or secondary schools in England. The purpose of this review is to inform recommendations about the use of screening programmes in schools to identify children at risk of or already experiencing mental health difficulties.
Aim and objectives
The aim of the work was to review the evidence for mental health screening and identification programmes based in schools and to judge whether current evidence fulfils selected UK National Screening Committee (UKNSC) criteria for the implementation of screening for mental health or risk of mental illness in those settings.
Methods
We sought to replicate the UKNSC evidence review process as far as was feasible for a single researcher, with support from Public Health England library services. A rapid review was conducted broadly according to Garritty et al (2020). This approach produces an evidence summary addressing a research question or set of questions in a priority topic area produced within a short timeframe (1 week to 6 months). Studies, identified by a search of nine databases, were screened according to predefined inclusion and exclusion criteria by a single reviewer (Figure 1), narratively synthesised and applied to the UK National Screening Committee criteria (UKNSC, 2015). A summary of evidence applied to the UK NSC criteria is presented in Table 1. The following studies were included:
- Systematic, scoping reviews and metanalysis – Anderson et al (2018), Deighton et al (2014), Johnstone et al (2018), PHE (2019), Runyon et al (2018), Soneson et al (2020), Sutan et al (2018), Stocking et al (2018)
- Non-systematic reviews – Dvorsky et al (2014), Newlove-Delgado and Ford (2020), Turner (2015)
- Other types of studies – Bowman et al (2016), Burns and Rapee (2019), Burns and Rapee 2016), Deighton et al (2013), Dowdy et al (2015), Dowdy et al (2013), Dwyer et al (2006), Finning et al (2020), Ford et al (2019), Gonzalez et al (2016), Kaess et al (2014), Kuo et al (2009), Martinsen et al (2019), Miller et al (2015), Renshaw (2017), Sinclair and Holden 2013), Wolf et al (2019), Wolpert et al (2013), von der Embse et al (2015), von der Embse et al (2017).
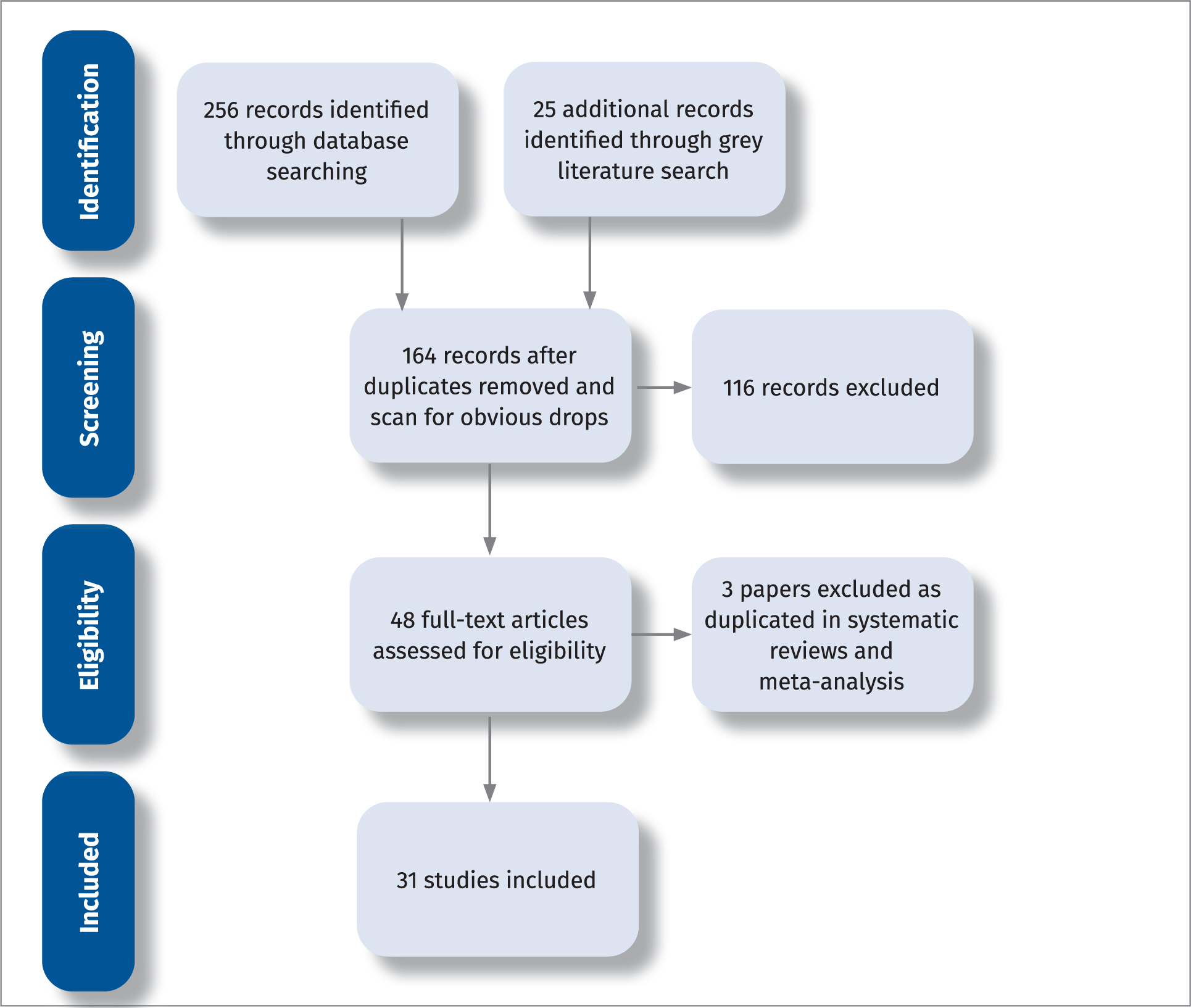
Table 1. Summary of evidence applied to the UK NSC criteria
| Criteria | Importance of health problem | Implementation of cost-effective primary prevention interventions | Simple, safe, precise, validated, acceptable screening test with suitable cut-off | Agreed pathway for further investigation | An effective intervention which is more effective if given early | RCT evidence for screening programme reducing morbidity and mortality | Feasibility and acceptability of the programme | Programme benefits outweigh harms | Value for money |
|---|---|---|---|---|---|---|---|---|---|
| Met? | ✓Good evidence was identified from UK surveys and the CMO report of the prevalence of MHD in children and the association between risk factors and psychiatric disorders in later life | XLimited evidence of universal interventions that consistently show a sustained, meaningful effect to improve children's mental health and wellbeing | Partially metThere are a variety of validated screening tools that are either broad or specific and dependent on the nature of the MHD. However, there is no consensus as to the most suitable, simple screening tool, screening age or frequency of screening in the school settings | XThere is limited evidence from the literature about the pathways from school-based screening into school-based support or CAMHS. | ✓Some evidence for effective interventions, dependent on the nature of the MHD, including school-based programmes and psychological interventions provided by NHS Child and Adolescent Mental Health Services (CAMHS).However, there are issues with access and waiting times, with MHSTs being introduced to help address this | XNo RCT evidence for MHD screening programmes' impact on morbidity and mortality | XSoneson et al's (2020) systematic review concluded the evidence for feasibility and acceptability of universal screening for mental health difficulties in school settings is mixed, also limited evidence from the UK | XLack of evidence on potential benefits and harms of programmes | XAnderson et al (2018) systematic review concluded there was a lack of evidence on the cost effectiveness of screening CYP for MH difficulties |
These studies are presented in more detail in separate tables in Appendix 1 [These can be requested by contacting the editor].
Summary of the findings
The condition
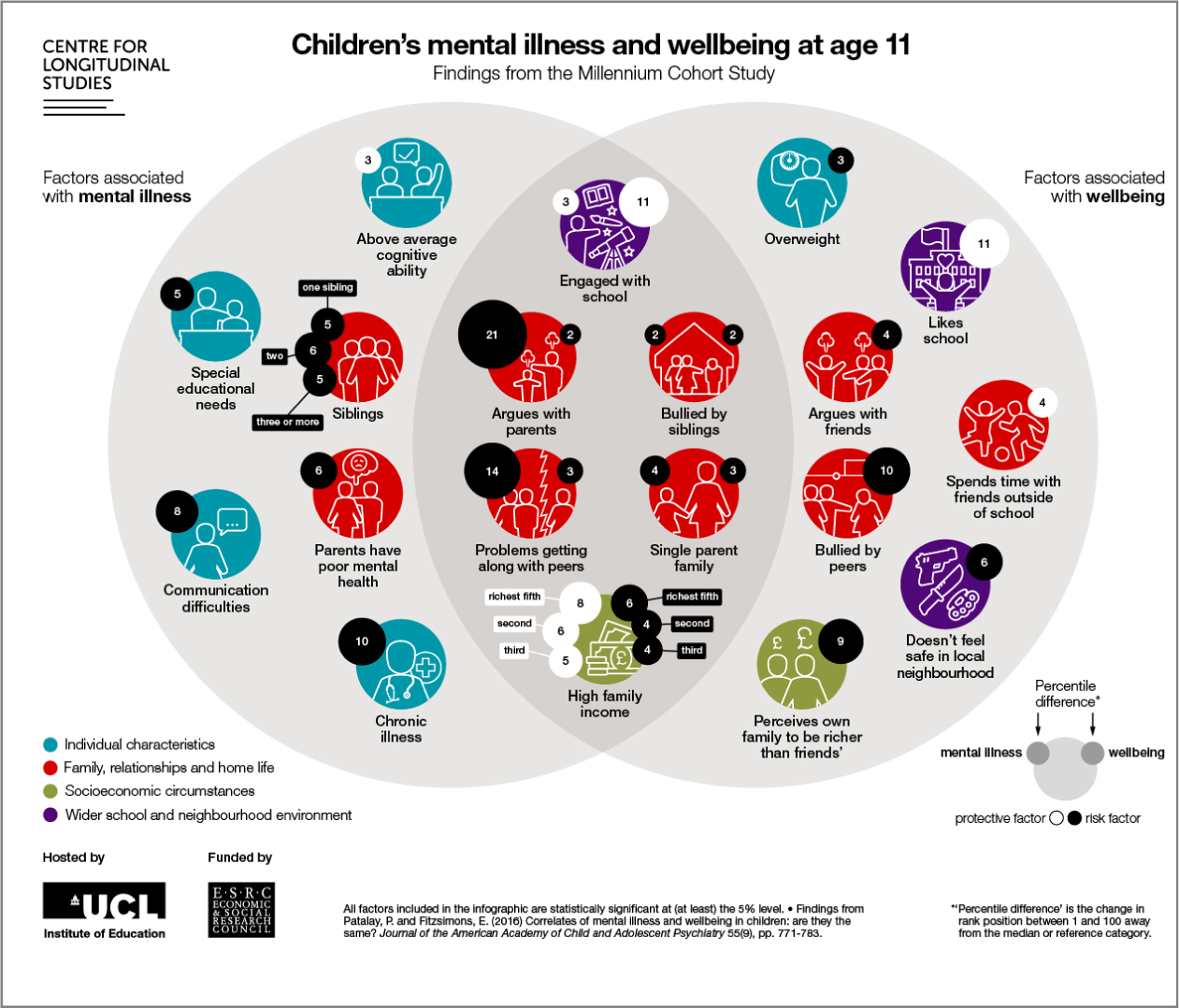
Good evidence was identified from annual surveys and longitudinal studies (CMO, 2012; NHS Digital, 2018; NHS Digital, 2020) that mental health difficulties affect a significant proportion of 5 to 19-year-olds and although any child can experience mental health problems, some children and young people (e.g. those experiencing social disadvantage and adversity) are at greater risk of developing mental health problems than others, whereas certain factors can act as protection (Figure 2).
For some psychiatric disorders, there is evidence that interventions early during the course of the disorder could shorten the duration or severity, as well as prevent or ameliorate adverse outcomes associated with the disorder (WHO, 2004; Newlove-Delgado and Ford, 2020). Additionally, if young people do not receive appropriate mental health treatment, they are at increased risk for later conduct problems, being involved in crime and experiencing severe mental health problems (CMO, 2013; Dvorsky et al, 2014; WHO, 2014). This evidence supports the notion that the condition (child mental health difficulties) is an important health problem. However, the literature reviewed did not address whether all the cost-effective primary prevention interventions have been implemented as far as practicable.
The test
There is no consensus as to the most suitable screening measure, and this review found that there are already multiple, validated mental health screening tools in use nationally and internationally that are either broad (i.e. assessing multiple domains) or specific (assessing only one domain), reflecting the range in nature of MHD from behavioural, emotional, hyperkinetic problems to different manifestations across the life course and by sex (Public Health England [PHE] and Anna Freud National Centre for Children and Families, 2016; Siceloff et al, 2017).
This review also identified several other screening instruments being tested for both their reliability and validity and trialled specifically for school-based assessment of mental health risk in children (Dwyer et al, 2006; Deighton et al, 2013; Von der Embse et al, 2016 and 2017; Burns and Rapee, 2016 and 2019; Renshaw, 2017). Studies identified by this review were also testing the use of several existing, validated instruments in schools (Kuo et al, 2009; Sinclair and Holden, 2013; Kaess et al, 2014; Gonzalez et al, 2016). Others were comparing different measures to screen for social, emotional, and behavioural risk (Miller et al, 2015) or whether the efficacy of existing validated tools was affected by the child's sex and by socio-demographic factors (Bowman et al, 2016).
The lack of a single, nationally recommended, freely available screening tool may present a significant barrier in terms of universal implementation, as schools report having limited personnel with adequate training or time to identify psychometrically sound universal screening measures (Siceloff, 2014). In the meantime, UK school staff are also using ‘bespoke questionnaires’ that may not have been validated for use in this manner, thus increasing the risks of under- or over-identification of mental health difficulties and of unintended consequences (Marshall et al, 2017; Newlove-Delgado and Ford, 2020)
The evidence for feasibility and acceptability was mixed. There was evidence screening for emotional and behavioural problems in school matched school staff priorities, but that staff did not necessarily view the identification of such problems as a school responsibility, although support from school staff increased, with increasing participation in screening programmes (Soneson et al, 2020). Flexible programmes were reported as more feasible, particularly when universal screening could be adapted to target higher-risk groups only (Soneson et al, 2020). Barriers to implementation included adequate supervision, additional human and material resources required, communication with parents and attainment of their consent (Conners et al, 2015; Soneson et al, 2020).
The intervention
A wide range of evidence-based and other ‘promising practice’ approaches and interventions were identified (see intervention Table 2).
Table 2. Interventions for children at risk of or already experiencing mental health difficulties, identified in school settings via a screening programme
| Level | Interventions | Description and examples | Evidence and source/s |
|---|---|---|---|
| Tier 1. Family, community and whole-school approaches to improving children and young people's mental health and resilience | |||
| Family | Parenting programmes | 5 pillars of parenting: a targeted-selected programme aimed at Muslim parents with a child between the ages of 4 and 11 years. | Early Intervention Foundation Guidebook – Evidence rating 2 5 Pillars of Parenting (4–11 years) has preliminary evidence of improving a child's outcome, but EIF cannot be confident that the programme caused the improvement. |
| Group Teen Triple P is a universal intervention for parents of an adolescent child, aged between 12–16 years. | Public Health England (2019c) Universal approaches to improving children and young people's mental health and wellbeing. The report of the findings of a special interest group who undertook a synthesis of systematic reviews to identify, synthesise and present key evidence of universal approaches to improving mental health and wellbeing of children and young people, with a view to informing policy and practice.Early Intervention Foundation Guidebook – Evidence rating 3 Level 4 Group Teen Triple P has evidence of a short-term positive impact on child outcomes from at least one rigorous evaluation. | ||
| Standard Teen Triple P is a targeted-indicated intervention for parents of an adolescent child, aged 12–16 years. | Early Intervention Foundation Guidebook – Evidence rating 2 Level 4 Standard Teen Triple P has preliminary evidence of improving a child outcome, but EIF cannot be confident that the programme caused the improvement. | ||
| Parents Plus Children's Programme (PPCP) is for parents with a child aged 6–11, with concerns about behaviour, learning or emotional development. | Early Intervention Foundation Guidebook – Evidence rating 2Parents Plus Children's Programme has preliminary evidence of improving a child outcome, but EIF cannot be confident that the programme caused the improvement. | ||
| Strengthening Families Programme 10–14 is a parenting and family strengthening programme for families with children aged 10–14. It can be implemented as a universal programme or targeted at high-risk adolescents. | Early Intervention Foundation Guidebook – Evidence rating 3Strengthening Families Programme 10–14 has evidence of a short-term positive impact on child outcomes from at least one rigorous evaluation. | ||
| Institution | School-based | Whole School Approach involves all parts of the school, working together and being committed to the health and wellbeing of students and staff (i.e. leadership and management, policy, overall school ethos, curriculum teaching and learning, staff training, identifying needs and monitoring outcomes, etc.)It needs partnership working between senior leaders, teachers and all school staff, as well as parents, carers and the wider community. | Promoting children and young people's emotional health and wellbeing, A whole-school and college approach - Guidance for headteachers and college principals on the 8 principles for promoting emotional health and wellbeing in schools and colleges (PHE, 2015)NICE (2009) Social and emotional wellbeing in secondary education, LondonNICE (2008) Social and emotional wellbeing in primary education, LondonNational Children's Bureau (2016) A whole-school framework for emotional wellbeing and mental health: a self-assessment and improvement tool for school leaders. |
| RSHE as a subject becomes compulsory from September 2020. However, schools were encouraged by the government to adopt the new curriculum from September 2019 onwards, so many schools will already be teaching the new subject. The subject is split into two sections: physical health and mental wellbeing, and relationships | Relationships and sex education (RSE) and health education – Statutory guidance for governing bodies, proprietors, head teachers, principals, senior leadership teams, teachers (DfE, 2019) | ||
| Incredible Years Classroom Management is a universal classroom management programme for teachers of children aged 4–8. | Early Intervention Foundation Guidebook – Evidence rating 3+ Incredible Years Teacher Classroom Management has evidence of a short-term positive impact on child outcomes from at least one rigorous evaluation. Ford T et al, (2019) evaluated the effectiveness and cost effectiveness of the programme and found the intervention reduced the SDQ-Total Difficulties score at 9 months for the intervention group, but this did not persist at 18 or 30 months. The intervention was particularly effective for children who were already struggling. | ||
| MindUP is a schools-based social and emotional learning and mindfulness programme. It is a universal programme and is offered in three versions pertaining to children aged 3–7 (MindUP 3–7), 8–11 (MindUP 8–11), and 11–14 (MindUP 11–14).MindUP 3–7 aims to improve self-regulation, pro-sociality in the short-term, and academic achievement and positive mental health in the long-term. | Early Intervention Foundation Guidebook – Evidence rating 2MindUP has preliminary evidence of improving a child outcome, but EIF cannot be confident that the programme caused the improvement.Systematic Review of School-Based Mental Health Intervention among Primary School Children – Mind UP was 1 of 9 interventions identified in a systematic review by Sutan et al (2018). They found almost all school-based mental health interventions in their review were proven to have a positive impact on mental health among school children, on the socio-emotional learning aspects including the social competency skill and cognitive control. | ||
| The Olweus Bullying Prevention Programme (OBPP) is a whole-school approach to bullying prevention, which is designed for students in primary and secondary schools (aged 5–18). All students participate in most aspects of the programme, while those who bully others and those who are bullied receive additional individualised interventions | Early Intervention Foundation Guidebook – Evidence rating 3+Olweus Bullying Prevention Programme has evidence of a short-term positive impact on child outcomes from at least one rigorous evaluation | ||
| The PATHS Elementary curriculum is a comprehensive programme for promoting emotional and social competencies and reducing aggression and behaviour problems in elementary school-aged children while simultaneously enhancing the educational process in the classroom. | Early Intervention Foundation Guidebook – Evidence rating 3+PATHS Elementary curriculum has evidence of a short-term positive impact on child outcomes from at least one rigorous evaluation | ||
| Rock and Water is a social and emotional learning programme for children and young people. It aims to improve skills such as self-regulation, communication and empathy. It can be delivered in a variety of settings, such as schools or youth clubs. | Early Intervention Foundation Guidebook – Evidence rating 2+Rock and Water has preliminary evidence of improving a child outcome, but EIF cannot be confident that the programme caused the improvement. | ||
| Community | Community strengthening | Community-centred interventionsStrengthening community actionsPlace-based approaches to reducing health inequalities (PHE 2019)Communities That Care (CTC) – multi-agency community programme | Wang et al, reported an association between neighbourhood disorder and Adverse Childhood Experiences.While this association may not be causal, further research is required on the role of community-based activities and place-based approaches to health inequalities for reducing ACEs |
| Universal campaigns | Promoting mental health and wellbeing and raising awareness/reducing stigma | Examples include.
|
|
| Reducing modifiable socioeconomic inequalities | Place-based approaches to reducing health inequalities (PHE 2019)Policy measures and guidelines | Childhood socioeconomic conditions have considerable influence on outcomes (Taylor-Robinson et al, 2018) | |
| Tier 2. School-based interventions to improve children and young people's mental health and resilience | |||
| Creating links to parents and services and sharing information once CYP identified via screening | Designated mental health leads in schools | The designated lead will
|
Promoting children and young people's emotional health and wellbeing – A whole-school and college approach (PHE, 2015)Transforming children and young people's mental health provision: a green paper(DH and DfE, 2017)Recommendations for effective school mental health programming indicate that all mental health services should be linked and coordinated (Dvorsky, 2014). |
| Interventions and programmes provided within the school setting | Child protection services/safeguarding | For vulnerable children | Safeguarding measures may be needed to identify and appropriately support vulnerable children and young people. |
| Healthy Child Programme: school nursing | For children and young people presenting with mental health difficulties, school nurses have traditionally provided face to face ‘drop in’ clinics in school settings and support via telephone/text/online, etc. Examples include Chat Health. | School aged years high impact area 1: Resilience and emotional wellbeing. School nurses leading the Healthy Child Programme 5–19 (PHE, 2018)0–19 health visiting and school nurses' services are commissioned by local authorities, the service provision and offer to schools will vary. Some areas have decommissioned school nursing services (King-Hicks and Jessup, 2020)Turner and Mackay (2015) The impact of school nurse interventions: behaviour change and mental health. | |
| School-based programmes | ‘Promising interventions’ identified by PHE included
|
Universal approaches to improving children and young people's mental health and wellbeing (PHE 2019)Universal approaches to improving children and young people's mental health and wellbeing – Findings from the synthesis of systematic reviews (PHE 2019)The 2019 report of the findings of a Special Interest Group who undertook a synthesis of systematic reviews to identify, synthesise and present key evidence of universal approaches to improving mental health and wellbeing of children and young people, with a view to informing policy and practice. Of the eight promising school-based interventions, four (FRIENDS, PATHS, and Penn Resilience [but only for Latino children]) had evidence showing a positive impact on a 12-month follow-up.A Meta-Analysis of universal school-based prevention programmes for anxiety and depression in children by Johnstone K, Kemps E. and Chen, J (2018) suggests that current anxiety and depression prevention programmes may be effective in preventing symptoms of depression at post-prevention and at long-term follow-up periods. However, no evidence was found to suggest that these programmes have an effect on anxiety symptoms.A systematic review of prevention interventions – universal, selective and indicated by Stocking et al (2016) found that these interventions were shown to reduce risk of disorder onset and reduce symptom levels for internalising disorders for up to 12 months. The authors suggest there is efficacy of large-scale implementation of prevention interventions in school settings, and within existing school-staffing resource is supported by existing studies.Early Intervention Foundation Guidebook (online)
|
|
| Nurture Groups – Classic Boxall Model is a short-term intervention grounded in Bowlby's attachment theory, which aims to address barriers to learning arising from unmet attachment needs. | Early Intervention Foundation Guidebook – Evidence rating 2+Nurture Groups has preliminary evidence of improving a child outcome, but EIF cannot be confident that the programme caused the improvement. | ||
| Pyramid Club is a targeted programme for children who are identified as being quiet, shy and behaviourally more likely to internalise. Pyramid Club Transition is provided to children transitioning to secondary school, with activity content and material tailored to this group. | Early Intervention Foundation Guidebook – Evidence rating 2+Pyramid Club Transition has preliminary evidence of improving a child outcome, but EIF cannot be confident that the programme caused the improvement. | ||
| Mental Health Support Teams | For children and young people presenting with mental health difficultiesMHSTs are a new service designed to help meet the mental health needs of children and young people in education settings. They:
|
Transforming children and young people's mental health provision: a green paper (DH and DfE, 2017)NHS Mental Health Implementation Plan 2019/20 – 2023/24MHSTs are relatively new and are currently rolled out in phases but not all CYP will have access: NHSE and I target is for 20–25% coverage by 2023/24 according to the NHS Mental Health Implementation Plan – 2019-20 – 2023/24 (NHS, 2019). Their effectiveness of MHST's is still to be evaluated. | |
| Psychological interventions provided by Child and Adolescent Mental Health Services (CAMHS) | For children and young people presenting with mental health difficultiesExample: EMOTION programme, provided in schools in Norway (so may not be applicable in the UK), was successful in reducing youth-reported symptoms of anxiety and depression and parent-reported depression, although the duration of the intervention effect was not reported. The programme uses CBT techniques and is provided by trained psychologists and school health nurses. | Evidence-based NHS treatment, trained professionals, utilising their clinical expertise and NICE GuidanceMartinsen et al (2019) Prevention of anxiety and depression in school children: Effectiveness of the transdiagnostic EMOTION program. | |
| Tier 3 and 4. Community-based services and specialist interventions | |||
| Individual and family | Psychological and pharmacological interventions | Child and Adolescent Mental Health Services (CAMHS) utilising evidence-based therapy (e.g. cognitive behavioural therapy [CBT]) | Evidence-based NHS treatment, trained professionals, utilising their clinical expertise and NICE GuidanceNICE (2015) Attachment difficulties in children and young people (NG26)NICE (2018) Attention deficit hyperactivity disorder: diagnosis and management: guidance (NG87)NICE (2015) Bipolar disorder, psychosis and schizophrenia in children and young people: QS102NICE (2019) Depression in children and young people: identification and management: guidance (NG134)NICE (2013a) Social anxiety disorder: recognition, assessment and treatment: guidance (CG159).NICE (2013b) Psychosis and schizophrenia in children and young people: recognition and management: guidance (CG155).Early Intervention Foundation Guidebook – Evidence rating 3Trauma-Focused Cognitive Behavioural Therapy has evidence of a short-term positive impact on child outcomes from at least one rigorous evaluation. |
Family, community and whole-school approaches to improving children and young people's mental health and resilience
In 2018-19 a mixed methods approach was undertaken by a PHE-led specialist interest group to understand the evidence for universal approaches to improving children and young people's mental wellbeing (PHE, 2019b). The report concluded that there was no clear evidence of evaluated universal interventions that consistently show a sustained, meaningful effect to improve children's mental health and wellbeing. However, the synthesis of systematic reviews (PHE, 2019c) commissioned to inform the work of the specialist interest group did identify 8 ‘promising practice’ interventions based on having at least 2 studies reporting positive outcomes, 7 of which have been included in Table 1. The lay summary report (PHE, 2019a) also identifies characteristics of the promising interventions, identified in the grey literature, operating at individual, family, and community levels. Of the promising interventions operating at a family level, common characteristics included whether they were provided online, supported by professional input, and involved skills-based practice.
Despite the lack of evidence identified in systematic reviews, the National Institute for Health and Care Excellence (NICE, 2009) advocates that schools adopt ‘an organisation-wide approach to promoting the social and emotional wellbeing of young people. This should encompass organisation and management issues as well as the curriculum and extra-curriculum provision’. The whole-school approach to promoting children and young people's emotional health and wellbeing is supported by a framework of eight principles outlined in national guidance for headteachers and college principals (PHE, 2015).
At a community level, campaigns promoting mental health and wellbeing, aiming to raise awareness and reduce stigma are widely used, while activities to strengthen communities and reduce inequity and health inequalities are acknowledged as important to prevent adverse childhood experiences and support children to thrive (PHE, 2020).
School-based interventions to improve children and young people's mental health and resilience
A systematic review of school-based mental health interventions among primary school children by Sutan et al (2018) concluded they had a positive impact on mental health among school children, on the socio-emotional learning aspects inclusive of the social competency skill and cognitive control. However, the authors acknowledge the suboptimal design of the 9 included studies and risk of bias.
Similarly, a ‘Meta-analysis of universal school-based prevention programmes for anxiety and depression in children’ (Johnstone et al, 2018) suggests that current anxiety and depression prevention programmes may be effective in preventing symptoms of depression at post-prevention and at long-term follow-up periods. The paper also cited that programmes which contained a greater number of sessions showed beneficial effects on anxiety and depressive symptoms. However, overall, the authors found no evidence to suggest that these programmes have a positive effect on anxiety symptoms.
The lay summary report (PHE, 2019a) identified the characteristics of the promising interventions, identified in the grey literature, operating at individual and school/community levels. They include the following key features:
- Provided in schools
- Offered in a group setting (often a class)
- Offered over a series of weeks from 10–24 often in 30 minutes to 1 hour
- Led by professionals (teachers or psychologists)
- Skills-based with strong emphasis on experiential practice in situ
- Often draw on cognitive behavioural therapy principles
- Often include an element of fun and enjoyable practice experiences.
Other school-based interventions include statutory safeguarding activities and school nursing services, who have traditionally provided face to face ‘drop in’ clinics in school settings and support via telephone/text/online, etc. A review exploring the impact of school nurse interventions relating to mental health and behaviour change found that although school nurse interventions resulted in a variety of positive outcomes for young people, in relation to emotional health and a variety of lifestyle outcomes, there was a reliance on descriptive reporting and a lack of formal service evaluation (Turner, 2015).
Forthcoming school-based interventions to improve support for children and young people's mental health include those outlined in Transforming Children and Young People's Mental Health Green Paper (DH and DfE, 2017). The role of a designated senior school lead for mental health is supported in the literature (Dvorsky, 2014, Public Health England, 2015) to enable the ‘Whole School Approach’, improving information sharing, coordination of services and links between parents and support services.
MHSTs are still relatively new and are currently rolled out in phases across England, but these are targeted programmes and not all CYP will have access. The NHSE and I target is for 20–25% coverage by 2023/24 according to the NHS Mental Health Implementation Plan – 2019/20 – 2023/24 (NHS, 2019) and the effectiveness of MHSTs is still to be evaluated.
The evaluation of Targeted Mental Health in Schools (Wolpert et al, 2013), a previous administration's nationwide initiative that funded mental health provision in schools for pupils at risk of or already experiencing mental health problems, found the programme had mixed outcomes.
Community-based services and specialist interventions for CYP mental health
Clinical Commissioning Groups (CCGs) are responsible for the provision of NHS Child and Adolescent Mental Health Services (CAMHS). However, the local service offer from a specialist CAMHS is different depending on where you live and waiting times can vary (NHS Digital, 2019).
The Children's Commissioner reported that children in England are repeatedly struggling to access help, are told they are not ill enough to qualify for services and are offered advice instead (Children's Commissioner, 2020). As the NHS Mental Health Implementation Plan (NHS England and Improvement, 2019) acknowledges, ‘There is still a lot of work to do to provide quality and timely mental health care for everyone who needs it, and to tackle inequalities in access, experience and outcomes.’
Given the range of ‘promising practice’ interventions identified at individual, family and school/community levels, and evidence-based NHS CAMHS commissioned by CCGs, there is evidence of an effective intervention for children and young people with existing mental health difficulties, including those who would be identified through a school-based screening programme. However, this is not necessarily in place and accessible for every child or young person who needs it and this provision should be fully understood in advance of any screening programme being introduced.
There is also insufficient evidence to conclude that interventions at a pre-symptomatic phase (i.e. before the behaviours exceed the threshold for a parent or teacher referral for services) leads to better outcomes for the screened individual compared with usual care. This is because none of the systematic reviews or studies identified reported on the outcomes of a mental health screening programme for the children and young people concerned, beyond the relative uptake of treatment services.
The programme
Despite the acknowledgement that failure to identify and address mental health difficulties early in life affects individuals' long-term functioning and wellbeing, this review identified very little evidence on the potential for universal mental health screening in schools to reduce morbidity and mortality and improve health and wellbeing.
Two linked systematic reviews (Anderson et al, 2018; Soneson et al, 2020) and individual evaluations of screening instruments and models predominately focused on the feasibility, acceptability, effectiveness and cost effectiveness of implementing the screening method, rather than the screening programme overall (including identification, referral and uptake of referral and treatment).
Although the reviews concluded that the evidence for the feasibility and acceptability of universal screening for mental health difficulties in school settings is mixed, parents, students and health professionals were supportive of school-based screening programmes (Soneson et al, 2020), in contrast to school staff, who did not view the identification of these difficulties as a school responsibility.
Few studies had explicitly examined the adverse events or harms of screening (Anderson et al, 2018). Newlove-Delgado and Ford (2020) have expressed concerns about the use of screening tools, arguing that the process of screening can raise anxieties among parents and children, and that false positives may occur. Also, as levels of psychopathology can fluctuate over different periods, screening at one point in time also risks over- or under-identification of mental health difficulties and the screening result (if negative) may be misused to deny access to further support.
Finally, Anderson et al (2018) undertook a linked systematic review of the effectiveness and cost effectiveness of school-based identification of children and young people at risk of, or currently experiencing mental health difficulties and concluded that ‘the heterogeneity of studies, the absence of randomised studies and poor outcome reporting make for a weak evidence base that only generates tentative conclusions about the effectiveness of school-based identification programmes’ (Anderson et al, 2018).
Implications for research and practice
Currently there is insufficient evidence to recommend a national screening programme to identify children at risk of or already experiencing mental health difficulties in school settings, when applying the UKNSC screening criteria. The UKNSC criteria are strict, were developed with physical health programmes in mind, and further work may be needed to support the application of such criteria for screening relating to the broad range of mental health domains.
There are already multiple, validated screening tools available but schools report having limited personnel with adequate training or time to identify psychometrically sound universal screening measures. There may be a role for local public health to provide education colleagues with further expertise, support and/or signposting to meet this gap. However, there remains a need for a national consensus on a brief, psychometrically strong tool that screens all children for their mental wellbeing and risk of developing a wide variety of mental health difficulties that is free, requires little or no training, and allows for use by multiple professionals, including those based in schools. Without this consensus and leadership, untrained and/or unsupported school leaders, teachers and their support staff may continue to use invalidated ‘bespoke questionnaires’ increasing the risks of under or over identification of mental health difficulties and of unintended consequences.
There is some evidence for the feasibility and acceptability of school-based screening programmes, particularly among parents, pupils, and health professionals. However, further UK research is needed to determine whether such screening programmes can have a positive impact on CYP mental health, morbidity and mortality, to provide enough evidence for schools to invest additional human and material resources to implement and sustain the programme. While acknowledging that the traditional methodical approach to capturing effects (i.e. randomised control trials) need to be revised for universal public health programmes, there is still a requirement for more robust evaluation of existing school-based screening programmes, particularly in terms of identification of children at risk of mental health difficulties, rates of referral to (and outcomes of) intervention services and the cost effectiveness of universal/targeted mental health screening versus other ‘ad hoc’ methods of identification.
Finally, too few studies have explicitly examined adverse events or harms from screening for MHD and UKNSC will only approve screening if there is enough evidence to conclude the benefits outweigh the harms. For example, as levels of psychopathology may fluctuate, screening at one point in time also risks over- or under-identification of difficulties, and there is a risk ‘referrals for further assessment or treatment’ to CAMHS are based on the result of the screening assessment alone.
Conclusions
Although good evidence was identified from UK surveys and the CMO report of the prevalence of MHD in children and the association between risk factors and psychiatric disorders in later life, the evidence for the feasibility and acceptability of universal screening for mental health difficulties in school settings is mixed, and there is limited evidence on the effectiveness and cost effectiveness of these programmes, with very limited evidence available from the UK. Although there is evidence of effective interventions if more children and young people are identified earlier, there is still a lot of work to do to provide quality and timely access to mental health care for everyone who needs it.
In addition to reaching an academic consensus on the most suitable tool appropriate to age and outcome, timing and frequency of screening children and young people in schools, further research is needed to determine whether such programmes can have a positive impact on mortality and morbidity and whether there are any potential harms from false positives or false negatives, the absence of follow-up interventions and support being put in place, etc. Therefore, any use of validated screening tools in UK schools should be accompanied by a clear pathway into early intervention services and a robust evaluation of the whole programme from identification, through to referral, uptake of mental health support and the outcome for those children and young people.
KEY POINTS
- Rates of probable mental disorders in children and young people in England are increasing.
- The UK Government's Green Paper on children and young people's mental health set expectations for schools to take a central role in the identification of and response to mental health difficulties.
- Systematic, universal school-based screening approaches could detect a greater proportion of CYP with mental health difficulties compared with less formal processes (i.e. ad-hoc teacher or parent identification).
- The evidence for the feasibility and acceptability of universal screening for mental health difficulties in school settings is mixed, and there is limited evidence on the effectiveness and cost effectiveness of these programmes.
- Based on application of available evidence to the UKNSC screening criteria, there is currently insufficient evidence to recommend the implementation of a national screening programme for children at risk of or already experiencing mental health difficulties in school settings.
REFLECTIVE QUESTIONS
- What are the benefits of screening for mental health difficulties in children and young people?
- What are the risks?
- If schools are implementing a screening programme, what governance arrangements should be in place?